
This publication is produced in partnership with Project UNITY’s Catalyst Academy Class of 2025, a student public health research and education program.
Abstract
Maternal mortality is a critical issue in the United States, particularly for Black women. This is not solely a medical concern, but rather, a public health emergency rooted in systemic racism, lack of access to care, and decades of inequality. In Clifton, Ohio, a significant portion of the Black female population is facing these barriers, and existing healthcare programs remain insufficient. The purpose of this paper is to better understand the underlying causes of maternal mortality among African American women in Clifton. We reviewed 29 scholarly articles about reproductive care from sources such as PubMed, the Centers for Disease Control and Prevention (CDC), and the National Institutes of Health (NIH). In addition, we interviewed leaders from organizations dedicated to maternal health and racial equity. Through this process, we identified four key contributors to Black maternal mortality: limited transportation, inadequate access to care, racial disparities in treatment, and relationship-based challenges. To address these issues, we propose a mobile health bus that will provide free prenatal and postnatal services directly to affected communities. Our goal is to not only help reduce maternal mortality in Clifton but to eventually expand the model to other underserved cities.
Keywords: Black maternal health, socioeconomic disparities, racial health disparities, public health interventions, prenatal care, mobile health clinics
Introduction
Maternal mortality, defined as the death of a woman during pregnancy or within one year of the end of pregnancy, is one of the clearest indicators of a region’s overall health and commitment to equity. It remains a persistent and alarming public health crisis, even in one of the wealthiest and most medically advanced countries in the world. Each year, hundreds of women in the United States die due to complications related to pregnancy and childbirth, many of which are entirely preventable. Despite advancements in medical technology and hospital systems, gaps in the quality and accessibility of maternal care remain. These gaps disproportionately affect Black women, who are over two times more likely to die from pregnancy-related causes than White women, regardless of income or education (Ohio Department of Health, 2023). Failing to address this issue leads not only to unnecessary deaths, but also severe health consequences (untreated pregnancy complications), social consequences (such as generational trauma and family instability), and financial consequences (such as higher emergency care costs and burdens on Medicaid and community programs).
Reproductive health encompasses physical, mental, emotional, and social well-being relating to the reproductive system. A key measure of this is the maternal mortality rate, which is influenced by factors like racial disparities, social determinants of health, and maternity care deserts which are areas with little or no access to birthing facilities or providers. Clifton, Ohio, a small neighborhood within Hamilton County, reflects these challenges. Though surrounded by healthcare infrastructure, residents still face barriers such as long travel times, insurance gaps, provider shortages, and limited culturally competent care. The main objective of this paper is to investigate maternal mortality and reproductive health inequities in Clifton through a public health lens. Using the socioecological model, the paper will examine individual, interpersonal, organizational, community, and policy-level influences, in order to propose an intervention: a mobile maternal health clinic that addresses these disparities. From this paper, readers can expect to learn about the roots of reproductive health disparities, the unique challenges Black women face in accessing care, and a locally grounded solution aimed at advancing equity.
The Importance of a Public Health Lens
The disproportionately high rates of maternal mortality among Black women in the U.S. are rooted in the social determinants of health, which were shaped by a long history of systemic oppression. In particular, redlining policies in the mid-20th century segregated Black communities and denied them critical investments. This led to lasting disadvantages in healthcare, transportation, and housing. These inequities still persist today, with generational impacts on neighborhoods, environmental conditions, and access to care, all of which contribute to elevated maternal mortality rates. The socio-ecological model helps uncover the deeper layers of these disparities and provides a framework to understand the various causes of maternal mortality among Black women. At the interpersonal level, provider-patient relationships often involve implicit bias and the dismissal of symptoms reported by Black women, leading to inadequate care. Many Black patients report feeling ignored or disrespected by healthcare providers (CDC, 2022). At the organizational level, inadequate postpartum follow-up increases the risk of complications. At the policy level, structural racism in healthcare, housing, and education systems continues to drive poor maternal health outcomes in Black communities.
Methods
We reviewed and analyzed 29 sources in detail, including peer-reviewed journal articles, government health reports, and local public health documents. Afterwards, our team created a list of organizations that addressed maternal mortality and racial inequity, locally and nationally. We then found the contacts of CEOs, Presidents, PR Heads, etc, and sent emails to schedule an interview. Two stakeholder interviews were conducted. During the interviews, we took notes and applied their insight to our project. Our plan of action was designed based on the patterns and gaps discovered while completing our literature review and stakeholder interviews.
Literature Review
Maternal mortality in the U.S. has shifted notably in recent years, declining from 32.9 deaths per 100,000 live births in 2021 to 18.6 in 2023, with rates stabilizing into 2024 (CDC, 2025a; CDC, 2023b). Despite this progress, major racial disparities persist. In 2023, Black women faced a maternal mortality rate of 50.3 per 100,000 live births —over three times that of White (14.5) Hispanic (12.4) and Asian (10.7) women (CDC, 2023a). These gaps exist regardless of education, income, or insurance status, pointing to systemic issues in healthcare access and quality (Njoka et al., 2023). Although mortality rates dropped for most groups between 2022 and 2023, the rate for Black women slightly increased, widening the racial gap (AP News, 2025). Furthermore, over 80% of these deaths are preventable and are often linked to hemorrhage, hypertension, and infection (Oduyebo et al., 2023).
Maternal mortality also disproportionately impacts older women. In 2023, women aged 40 and older experienced a rate of 59.8 deaths per 100,000 live briths—nearly five times higher than women under 25 (Hoyert, 2023). This elevated risk is not only influenced by chronological age, but also by the long-term effects of chronic stress. Allostatic load, or the cumulative physical toll of chronic stress, accelerates biological aging. As a result, Black women can age biologically up to 10 years faster than White women, placing them at a greater maternal risk even at younger ages. (Katella, 2023). Additionally, 65% of maternal deaths occur postpartum, when risks of complications like severe bleeding, infection, and cardiomyopathy remain high (Gunja et al., 2024). Alongside this, compared to other countries, U.S. women receive limited postpartum care, with few home visits and no guaranteed paid leave, increasing the risk of maternal mortality overall.
Economic stability and access to quality healthcare also stand out as main contributors to maternal mortality disparities, under the Healthy People 2030 framework. Almost 36% of U.S. counties lack adequate obstetric services, leading to “maternity care deserts,” that disproportionately impact rural and marginalized communities (Adashi et al., 2024). Women living in these areas experience longer travel times, averaging 25 to 33 miles, to access obstetric care, which delays prenatal screening and management (Fontenot et al., 2024). Additionally, implicit bias from providers, along with structural racism within healthcare settings, significantly contribute to unequal treatment and the dismissal of Black women’s concerns, worsening adverse maternal outcomes (Montalmant & Ettinger, 2024)
Focusing now on Clifton, Ohio, Clifton is a small community situated in Hamilton County; consequently, public health data specific to this community is limited, and analyses typically rely on broader county or state-level reports. While there is limited direct data for Clifton itself, trends from nearby counties and Ohio help explain the broader reproductive health situation.
Looking now broadly at Ohio, maternal health outcomes show ongoing disparities. Between 2008 and 2016, the state had a maternal mortality rate of 14.7 deaths per 100,000 live births, with more than half of these deaths being preventable (Ohio Department of Health, 2019).
Black women in Clifton, Ohio, are most at risk. They are 2.5 to 3 times more likely to die from pregnancy-related causes than White women (Cincinnati Enquirer, 2022). This large gap shows that race plays a major role in maternal health, regardless of personal choices. From 2008 to 2016, the maternal mortality rate for Black women in Ohio was 29.5 per 100,000 live births, compared to 11.5 for White women (Johns Hopkins Center for Maternal and Child Health, 2021). These numbers reflect long-term systemic problems, including racism in healthcare, unequal access to services, and economic inequality. Neighborhoods like Clifton also experience higher rates of poverty and fewer medical resources, making it more challenging for women to get proper care (Cradle Cincinnati Annual Report, 2021).
Other personal factors such as education, income, and stress all play a role in maternal health outcomes. For instance, black women with less education often start prenatal care late. The CDC reports that only 70% of black women with a high school education or less begin care in the first trimester, compared to over 90% of women with college degrees (CDC, 2022). In Hamilton county, early care makes it easier to address health problems, start treatment, and ultimately prevent complications (March of Dimes, 2023). Additionally, financial stress and food insecurity are linked to serious issues such as hypertension and early pregnancy labor (American Psychological Association, 2023). Lack of transportation and low health literacy also prevent many women in rural areas like Clifton from getting consistent care.
Support from family, partners, and friends plays a vital role in improving maternal health by helping pregnant individuals attend medical appointments and follow healthcare guidance (WHO, 2023). Without this support system, women often experience increased stress and are more vulnerable to mental health challenges. According to the CDC, approximately 1 in 8 women suffer from postpartum depression (2023), a risk that is amplified in the absence of emotional or practical assistance. In rural or tight-knit communities, stigma surrounding reproductive health may further discourage women from seeking help. Additionally, studies have shown that Black women’s concerns are more frequently dismissed by healthcare professionals, contributing to poorer maternal health outcomes (March of Dimes, 2021). Institutions like hospitals and workplaces also shape reproductive health. Since many counties in Ohio, including Hamilton, are considered “maternity care deserts”, this forces pregnant people to travel long distances to get routine checkups or emergency care, worsening outcomes. On top of this, many workplaces do not offer paid maternity leave or health insurance, making women in these jobs more likely to delay care or miss appointments (Kaiser Family Foundation, 2020).
In Cincinnati, community groups are working to improve outcomes. Cradle Cincinnati gives free rides to doctor visits, home check-ins, and pregnancy support in neighborhoods like Clifton (Cradle Cincinnati, 2023). Queens Village focuses on building support for Black women and providing mental and reproductive health services (Queens Village, 2023). Local providers like UC Health and the Cincinnati Health Department also help women before and after birth. Many of these programs offer free wellness activities ultimately reducing stress and building a support system during pregnancy.
Recent policy changes have also assisted in making mild progress. Ohio now provides Medicaid coverage for 12 months after birth (Ohio Medicaid, 2023), giving new mothers more time to access care. Programs like Cradle Cincinnati receive support from local governments to continue their services. While all of this has proven incredibly beneficial, the aforementioned struggles of maternity call for more to be done. Hospitals could require training to reduce bias, Medicaid could cover doulas, and mental health services could be expanded. These steps would help make maternal care safer and more equitable for all women, especially those most at risks. Which raises the question: How do we transport this care?
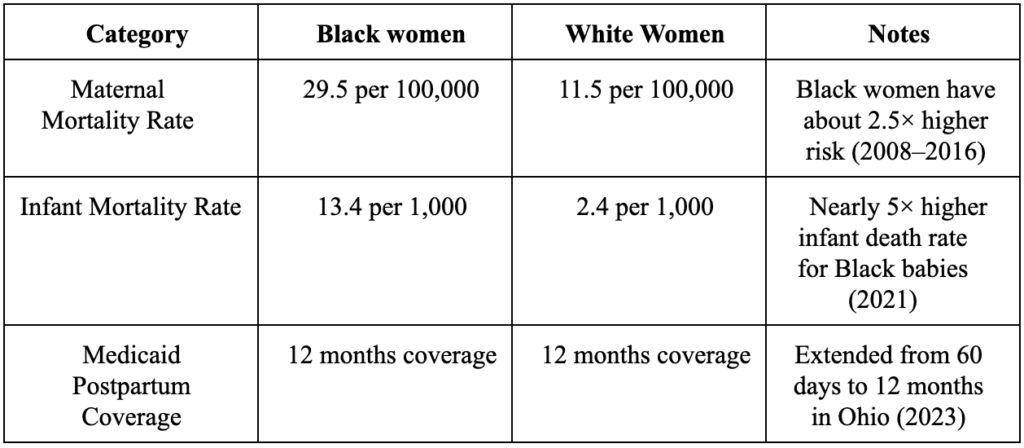
Table 1: Overview of Maternal Health Issues in Hamilton County (Hamilton County Public Health, 2023)
Table 2: Existing Maternal Health Programs in Hamilton County (Clifton, OH)
Stakeholder Perspectives
Our intervention was significantly shaped by our discussions with stakeholders, Chanetta Cottrell and Charla Hale. They both underlined that reducing maternal mortality requires addressing more extensive systemic gaps in access and education in addition to providing direct services. In communities like Clifton, Cottrell, of the Hamilton County Public Health Maternal and Infant Vitality Initiative, emphasized the effects of inadequate transportation and a lack of social support, pointing out that Medicaid transportation frequently falls short. To address this,her team links women with local navigators and resources, along with promoting hospital certifications that are doula-friendly.Healthy Moms and Babes President and CEO Hale described how the organization’s mobile unit integrates prenatal education, pregnancy testing, and case management with extended job and educational assistance for up to three years postpartum. This model demonstrates how sustained, community-based support can address gaps in maternal healthcare access while also mitigating socioeconomic barriers that influence maternal and infant outcomes. Through extending services beyond childbirth, the program promotes continuity of care, strengthens maternal stability, and recognizes the interdependence of health, education, and economic security in improving long-term family well-being. Strong collaborations with hospitals, Medicaid providers, and neighborhood organizations are the foundation of their success in attaining low infant mortality and high full-term birth rates. In order to effectively address maternal health disparities in underserved neighborhoods, these discussions collectively reaffirmed the significance of combining clinical services with community engagement, bias education, and resource accessibility.
Digital Health Solutions
The Quintuple Aim model demonstrates the importance of health equity and value-based care in improving healthcare. Developed in 2020, it serves as a framework for improving population outcomes, reducing healthcare costs, enhancing patient and provider experiences, and advancing health equity (Primary Health Network, 2024). Specifically, to address maternal mortality, applying the Quintuple Aim model is quite relevant since maternal mortality is a community health issue. In order to address it, attention must be paid to enhancing maternal health outcomes at the population level. This closely relates to the model’s “improving population health” component.
Alongside this, Digital Health can improve maternal health outcomes by advancing health equity and enhancing patient experiences. For instance, by implementing virtual visits and a hotspot on our mobile clinic, we aim to improve access to care for those who have busy schedules and have limited access to reliable internet. Below is a table explaining our digital health integration.
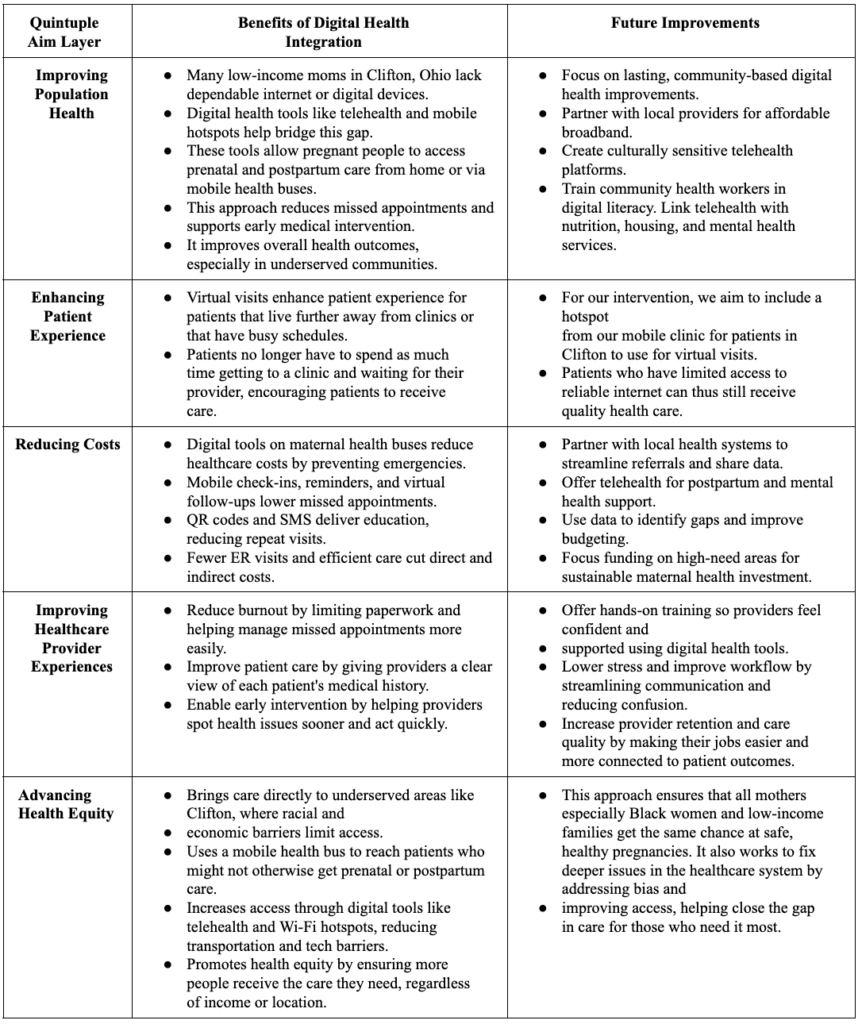
Table 3: Quintuple Aim Model and Maternal Mortality in Hamilton County, OH
Plan of Action
Target Population: This intervention seeks to support Black pregnant postpartum women, specifically targeting those 40 and older in Clifton, Ohio.
Goals: Through M.A.M.A, Mobilizing Activism for Maternal Access, we hope to reduce maternal mortality, improve healthcare access and tackle implicit bias in healthcare providers in Hamilton County.
Objectives: To do so, we aim to meet the following objectives:
– Within 6 months, have at least 25 providers attend a “Bias In Healthcare” workshop.
– Within the same 6 month period, serve at least 50 women through the mobile clinic.
– Within a year, distribute 50 post-partum bracelets to new mothers.
Intervention: Our intervention will utilize a collaborative mobile health model with OhioHealth’s Mom & Baby Mobile Health Center and Hamilton County’s 513 Relief Bus, to address maternal bias and healthcare disparities in underserved populations in Clifton, OH. This program makes use of a mobile clinic that makes monthly visits to the Clifton community to provide clinical services and focused educational programs in an approachable, culturally sensitive way.
Distributing maternal identification bracelets during mobile clinic visits serves as a targeted intervention for new mothers by providing immediate identification, facilitating continuity of care, and supporting access to follow-up services across healthcare and social service settings. These bracelets, with the words “new mom” printed on them, are designed to help prioritize prompt, courteous care in hospital and emergency department settings, by acting as a visual indicator of maternal status. We hope that mothers will wear these bracelets 6 weeks postpartum to create a concrete and easily identifiable marker, ultimately lessening the effects of implicit bias and enhancing patient advocacy.
Simultaneously, the mobile unit will conduct workshops titled “Bias in Healthcare,” which aim to teach community members to identify and deal with bias in medical settings. These workshops promote empowerment and health literacy by involving participants in interactive discussion and real-world scenarios. For those working in the buses, this will be a crucial step in preventing unconscious bias.
This multifaceted approach specifically addresses systemic bias, education, and access barriers. Through combining clinical outreach with visual prioritization tools and community involvement, the intervention aims to create long-lasting healthcare support networks in Clifton, foster community trust, and improve maternal and child health outcomes.
The program will require support from several local partners. While mobile health centers will conduct clinic visits and distribute maternal identification bracelets, partnerships with local hospitals and emergency departments are necessary to ensure staff recognize the bracelets and respond appropriately. This includes using the bracelets to identify recent postpartum patients, prioritize maternal health assessments, and facilitate timely referrals or follow-up care when mothers present for treatment.Community groups like churches, health workers, and neighborhood centers can help spread the word and encourage people to attend the workshops as well. It would also be helpful to work with local colleges or public health programs to help run the workshops and keep track of how beneficial the program is for the community.
To know if the intervention is working, we would collect feedback from both the moms and the healthcare workers. Surveys before and after the workshops could show if people are more confident in handling bias or feel more respected during doctor visits. We would also track data such as how often the mobile clinic is used, how many bracelets are given out, and whether emergency care is faster for those wearing bracelets. Interviews or feedback from hospital staff could help us understand if they are noticing changes too. This kind of information will show if the program is making a real difference in the community.
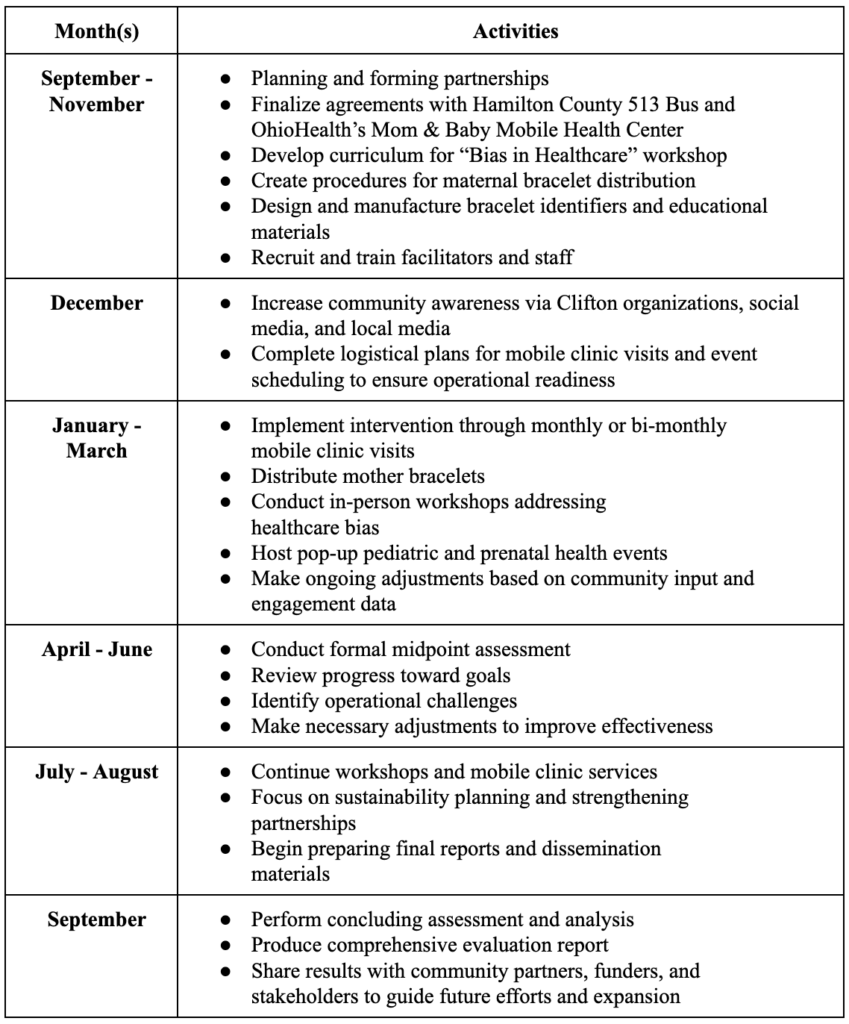
Table 4: Timeline for Implementation of M.A.M.A.
Several potential barriers to effective implementation have been identified, along with strategies to maintain the program’s integrity and reach:
We will collaborate with local leaders, churches, and utilize tools like town halls and social media to increase awareness and build trust within the community. If challenges arise with accessing the mobile unit or scheduling appointments, alternative sites and transportation assistance will be provided. To ensure hospitals implement the bracelet system effectively, staff and volunteers will receive early training and ongoing support. Recognizing the importance of cultural and linguistic accessibility, community health workers familiar with local backgrounds will conduct multilingual workshops and provide personalized support. In the event of a public health emergency, such as an outbreak, programming will shift to virtual formats or follow health and safety protocols to ensure continuity.
Resource Allocation
To successfully implement the intervention, several key resources are required: a mobile clinic serving Clifton, Ohio; medical professionals to staff the clinic; and postpartum bracelets for distribution to new mothers. The mobile unit will be supplied by our partner, OhioHealth’s Mom & Baby Mobile Health Center. Funding for both the clinic and medical personnel will come from another partner, Hamilton County Public Health. Our custom postpartum bracelets, produced by Wristbrand Bros, will cost approximately $141 for the first 150 units. We intend to secure funding for the bracelets through Project Unity. Additionally, for our “Bias in Healthcare” events, Mama Certified will provide the venue and curriculum. We will collaborate with them to coordinate guest speakers and ensure smooth event planning.
Strengths & Limitations
This intervention uniquely promotes reproductive health access and quality in Clifton, Ohio. By partnering with local organizations, we are able to build upon existing community relationships, infrastructure and programs. This enhances the impact and sustainability of the intervention.
In addition, inspired by the Institute for Healthcare Improvement, our implementation of the postpartum bracelets would be a completely innovative system in Hamilton County. According to USA Health, the postpartum bracelet initiative conducted by the Institute for Healthcare Improvement has the potential to significantly reduce maternal mortality by raising awareness of underlying health conditions in new moms (2023). Our intervention, however, faces a few challenges. One is getting hospitals and healthcare providers to support our program, and promote tools like our awareness bracelets. We also need to find enough trained professionals to staff the mobile clinic and offer consistent care. Other big challenges include funding the clinic, equipment, and digital tools. Finally, limited awareness within Clifton could significantly reduce clinic utilization.
To address this, outreach efforts will focus on trusted community channels rather than broad messaging. Collaborations with local leaders and churches, supported by targeted town halls and neighborhood-based social media outreach, will leverage existing networks of trust to disseminate information about clinic services and events. Through embedding outreach within established community structures, the program increases credibility, improves attendance, and ensures services reach mothers most likely to benefit.and health programs to find volunteers, and apply for grants or work with community organizations to raise funds. To spread awareness, we will use flyers, social media, and connect with local churches to help get the word out.
Discussion
Maternal mortality continues to affect Black pregnant and postpartum women in Clifton, Ohio at disproportionate rates. This issue is especially pressing for women over the age of 40, who face increased risk due to both medical and systemic factors. Many of these outcomes are shaped by barriers like limited access to care, deep-rooted bias in healthcare, and lack of community trust in medical systems. Addressing these challenges means going beyond clinical treatment to consider the social conditions that impact how women receive and experience care.
Our intervention brings healthcare directly into the community through a mobile unit that visits Clifton regularly. In partnership with trusted providers, this clinic offers essential maternal care in a setting that feels approachable and safe. During each visit, we distribute maternal ID bracelets that help mothers receive timely care in hospitals by signaling their pregnancy or postpartum status. We also offer workshops that focus on recognizing and addressing bias in medical environments. These sessions are designed to support both healthcare workers and community members by encouraging open dialogue and building confidence in navigating healthcare systems.
This work reflects the shift toward more inclusive, equitable healthcare. It aligns with the goals of improving population health and building trust between patients and providers. The digital components, including support for telehealth and technology access, help ensure continuity of care for those who cannot attend in person. By building on what already exists and adding tools that address the real experiences of Black mothers, this intervention offers a sustainable way to improve maternal health outcomes. Community feedback will guide how the program grows over time, helping us remain responsive and effective. The goal is not only to prevent deaths but to build a stronger, more supportive system of care that continues long after the first year.
Conclusion
Maternal mortality is a global critical public health issue, especially in Black and low-income communities. Limited access to care worsens health outcomes in both urban and rural communities, outcomes which are highlighted in Clifton, Ohio.
Our solution aims to reduce maternal deaths by improving healthcare access and quality. Initially, we would like to start in small towns like Clifton by implementing a mobile clinic that passes once a month. With this clinic, we will introduce “bias in healthcare” events to address implicit bias in providers and distribute “new mom” bracelets to postpartum mothers to raise awareness of underlying complications. Later on, we plan to expand to cities also experiencing high maternal mortality rates such as Philadelphia and New York City. As we expand nationally, we hope to have our “new mom” bracelets recognized by hospitals and providers.
Over time, this project has the potential to completely reshape maternal care across the U.S. by focusing on preventative care for postpartum mothers, promoting access to healthcare and addressing racial disparities.
References
- American Psychological Association. Stress and pregnancy. https://www.apa.org/topics/pregnancy/stress (2023).
- AP News. Racial gap widened in deaths among US moms around the time of childbirth. https://apnews.com/article/maternal-mortality-black-women-cdc-2023-9d6f1b6a1e8c4fbb 9f416ecb4b7b0a13(2025).
- Centers for Disease Control and Prevention. Prenatal care. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/prenatal-care.htm (2022).
- Centers for Disease Control and Prevention. Postpartum depression. https://www.cdc.gov/reproductivehealth/depression/index.htm (2023).
- Centers for Disease Control and Prevention. Maternal mortality rates in the United States, 2022. https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2022/maternal-mortality-rates-2 022.htm (2024).
- Centers for Disease Control and Prevention. Maternal mortality rates in the United States, 2023. https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2023/maternal-mortality-rates-2 023.htm (2025).
- Commonwealth Fund. Insights on the U.S. maternal mortality crisis in international comparison. https://www.commonwealthfund.org/publications/issue-briefs/2024/jun/insights-us-mater nal-mortality-crisis-international-comparison (2024).
- Cradle Cincinnati. Cradle Cincinnati. https://www.cradlecincinnati.org/ (n.d.).
- Cradle Cincinnati. Queen’s Village Cincinnati. https://www.cradlecincinnati.org/queens-village (n.d.).
- Cradle Cincinnati. Reducing infant mortality in Hamilton County. https://www.cradlecincinnati.org (n.d.).
- Guttmacher Institute. Sex and HIV education. https://www.guttmacher.org/state-policy/explore/sex-and-hiv-education (2023).
- Hamilton County Public Health. 2023 Maternal and Child Health Snapshot: Hamilton County. https://www.hcph.org/wp-content/uploads/2023/01/MCH_Snapshot_2023.pdf (2023).
- Hamilton County Public Health. Infant Maternal Health & Mortality – Hamilton County Public Health. https://hamiltoncountyhealth.org/services/health-promotion-education/infant-maternal-he alth-mortality/(2024).
- Health Department. Health. https://www.cincinnati-oh.gov/health/ (n.d.).
- Joseph, K. S. et al. Maternal mortality in the United States: Are the high and rising rates due to changes in obstetrical factors, maternal medical conditions, or maternal mortality measurement? Am. J. Obstet. Gynecol. S0002-9378 (2024). https://www.ajog.org/article/S0002-9378(24)00005-X/fulltext
- Kaiser Family Foundation. Health coverage of women. https://www.kff.org/womens-health-policy/fact-sheet/health-coverage-of-women/ (2020).
- Katella, K. Maternal mortality on the rise. Yale Medicine https://www.yalemedicine.org/news/maternal-mortality-on-the-rise (2023).
- Lorch, S. A. et al. Maternity care deserts and pregnancy-associated mortality in the USA. JAMA 331, 325–334 (2024). https://pubmed.ncbi.nlm.nih.gov/40268316/
- March of Dimes. Racial disparities in maternal health. https://www.marchofdimes.org/news/maternal-mortality-racial-disparities-persist.aspx (2021).
- March of Dimes. Ohio report card. https://www.marchofdimes.org/peristats/reports/ohio/report-card (2023).
- National Rural Health Association. Maternity care deserts. https://www.ruralhealthweb.org/programs/maternal-and-child-health/maternity-care-deser ts (2022).
- Njoka, A. C. et al. Racial disparities in U.S. maternal mortality: An updated review. Am. J. Obstet. Gynecol. 229, 15–22 (2023). https://pubmed.ncbi.nlm.nih.gov/36767014/
- Ohio Department of Medicaid. https://medicaid.ohio.gov/ (n.d.).
- Oduyebo, T. et al. Pregnancy-related deaths: Causes and preventability in the United States. Lancet Reg. Health Am. 21, 100552 (2023). https://pubmed.ncbi.nlm.nih.gov/37957536/
- Primary Health Network. The quintuple aim: Improving health equity for regions & communities. https://thephn.com.au/news/the-quintuple-aim-improving-health-equity-for-regions-communities (2024).
- Smith, D. B., Hardeman, R. R. & Chambers, B. D. Structural racism and maternal health disparities: A review of causes and solutions. Obstet. Gynecol. Clin. North Am. 50, 1–14 (2023). https://pubmed.ncbi.nlm.nih.gov/37957536/
- UC Health. Home (English). https://www.uchealth.com/ (n.d.).
- Uribe-Leitz, T. et al. Association of travel distance to obstetric services with prenatal care and maternal outcomes. JAMA Netw. Open 7, e246582 (2024). https://pubmed.ncbi.nlm.nih.gov/38720255/
- USA Health. Medical bracelets for new moms have the potential to save lives. https://www.usahealthsystem.com/news/medical-bracelets-new-mothers (2023).
- Watson, M. New Mama Certified program promotes safer, more equitable care for birthing parents. Cincinnati Business Courier https://www.bizjournals.com/cincinnati/news/2022/10/26/mama-certified-safer-care.html (2022).
- World Health Organization. Maternal mortality. https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (2023).
- World Health Organization. Social support during pregnancy. https://www.who.int/publications/i/item/social-support-during-pregnancy 24 (2023).
Related Posts

To safeguard Africa’s topmost predators
From Nepal’s bengal tiger to Kenya’s big Lions, conservation of...
Read More
The Public Health Humanitarian Crisis in Ukraine
This publication is in proud partnership with Project UNITY’s Catalyst Academy 2023...
Read More
Antimicrobial Resistance in Underprivileged Communities
This publication is in proud partnership with Project UNITY’s Catalyst...
Read More
The Geography of Disease: a Bayesian Approach to Epidemiology
Figure 1: A map showing relative rates of pancreatic cancer...
Read More
Autism Spectrum Disorder and Gender: The Case for Expanding the Autistic Phenotype
This article was originally submitted to the Modern MD competition...
Read More
Transgender Health Disparities in Prisons
Transgender people are targets for victimization within the prison system...
Read MoreDarius Dastur, Mishal Ali, Harshitha Ezhilarasan, Hasan Khan, Aaron Akasala