
This publication is produced in partnership with Project UNITY’s Catalyst Academy Class of 2025, a student public health research and education program.
Abstract
Sickle cell disease (SCD) is an inherited blood disorder affecting approximately 100,000 individuals in the United States, with the highest prevalence among African American populations. The disease is characterized by malformed red blood cells, which lead to organ damage and increased risks of infection. Due to its lifelong complications and need for continuous medical management, SCD presents significant challenges. Addressing SCD from a public health perspective is critical for improving early detection, enhancing disease management, and reducing health inequities worldwide.
The objective of this paper is to examine local SCD prevalence, identify key social determinants of health in View Park–Windsor Hills, California, and to develop a community-based intervention. Data was collected from peer-reviewed articles sourced from PubMed, the National Institute of Health, and Google Scholar with a focus on epidemiology, health disparities, and community outreach programs.
The findings reveal that Windsor Hills lacks specialized SCD clinics, experts, and awareness of the disease, which limits preventive care and continuity of treatment. Families often experience delays in emergency care and inconsistent follow-up due to the lack of healthcare resources. Existing interventions fail to address and support the needs of patients. The proposed intervention integrates SMS-based communication to support routine checkups and crisis management. Additionally, partnerships with schools and churches aim to connect patients with specialists at different local clinics. Together, these measures seek to improve long-term health conditions and reduce complications associated with SCD within the community.
Keywords: Sickle cell disease; health equity; healthcare access; View Park Windsor–Hills; health policy; social determinants of health
Introduction
Sickle cell disease (SCD) is a genetically inherited blood disorder that disproportionately affects individuals of African descent. People with SCD have abnormally shaped red blood cells that can obstruct the flow of blood and oxygen throughout the body. Because SCD is inherited, it is more prevalent in communities with a higher proportion of African American individuals. Those living with SCD face serious health challenges, while those with sickle cell trait remain asymptomatic and gain partial protection from malaria. Historically, malaria was widespread in sub-Saharan Africa, and individuals with sickle cell trait were more likely to survive malaria infections, leading to a higher prevalence of the sickle cell gene among populations of African descent through natural selection. This evolutionary advantage explains the strong association between the sickle cell trait and African ancestry.
This study focuses on View Park–Windsor Hills, located in Los Angeles County, California, due to its large African American community. By examining this community, this research aims to shed light on the health challenges faced by residents living with SCD, and to promote greater awareness, informed decision-making, and targeted interventions to improve access to care and overall quality of life.
We begin by discussing the importance of a public health lens through exploring the social, structural, and behavioral determinants that shape SCD outcomes and underscore the need for multifaceted approaches. The methods section outlines how data analysis, community needs assessments, and evidence-based frameworks informed the design of our intervention. In the literature review, we synthesize current research on SCD disparities and identify strategies to strengthen our proposal. The stakeholder perspectives section highlights the critical roles of healthcare providers, community leaders, and policymakers in ensuring successful implementation. Additionally, we present digital health solutions, including SMS reminders and community engagement strategies to support self-care and disease self-management. Our plan of action details the steps for implementation, while the strengths and limitations section critically examines the feasibility and challenges of our approach. Finally, the discussion section reflects on broader implications, policy recommendations, and opportunities to improve outcomes for the wider community.
Public Health Lens
The prevention and management of sickle cell disease (SCD) requires approaches that extend beyond individual clinical treatment. SCD must be addressed through a public health framework, as it enables the development of population-level strategies, which include genetic factors like family history and ancestry, while also addressing socioeconomic factors that limit access to care. Understanding SCD in the context of broader social, economic, and environmental causes is essential for giving a panoramic view on the diagnosis of SCD. Public health efforts aimed at primary prevention and early intervention, such as newborn screening and prophylactic medications and immunizations (Kuznik et al., 2016), have the potential to reduce overall disease burden and improve quality of life for individuals living with SCD. Furthermore, the public health framework emphasizes health education and awareness campaigns, which can empower communities with the knowledge and resources necessary to support behavioral changes and encourage timely access to medical care. These efforts are particularly important for reducing health disparities and ensuring that vulnerable populations, including African Americans, have equitable access to preventive services and care (Lee et al., 2019).
The socio-ecological model describes the relationships among groups through multilevel factors. At the individual level, genetic inheritance is the primary cause of sickle cell disease, while external factors such as stress and exposure to extreme temperatures can exacerbate SCD. At the interpersonal level, strong relationships with a support group may help reduce the impact of sickle cell disease. At the organizational level, the quality and accessibility of healthcare services play a critical role in disease treatment. At the community level, social conditions such as housing quality and educational attainment significantly influence health outcomes as well. Finally, at the policy level, Medicaid funding and insurance coverage policies for SCD directly affect access to treatment. By analyzing the disparities across differing levels, the socio-ecological model offers valuable insight into how public health systems can be improved to better serve affected individuals and communities in need.
Methods
A comprehensive literature review on Sickle Cell Disease (SCD) was conducted using 37 sources, including the Centers for Disease Control and Prevention (CDC), the National Institutes of Health (NIH), UCLA Health, the National Heart, Lung, and Blood Institute (NHLBI), and peer-reviewed journals accessed through Google Scholar. These sources provided detailed information on population health statistics, risk factors, disease prevalence, and health trends related to the effects of SCD in California, with a specific focus on Los Angeles County. This geographically targeted search allowed for close alignment between the data and the population and healthcare systems under investigation, ensuring precision and contextual relevance through the use of reliable and region-specific sources. One stakeholder interview was conducted with the Foundation for Sickle Cell Disease Research via Zoom. Stakeholders were identified based on their demonstrated commitment to advancing sickle cell research and improving access to programs throughout the community.
To address the daily and systemic challenges faced by individuals living with SCD, particularly within an underserved community like View Park–Windsor Hills, a low-cost, accessible intervention grounded in public health education and community trust was developed. The core of the initiative is a multicomponent care kit distributed through community hubs such as hospitals, schools, and churches. Each kit includes a reusable water bottle with hourly hydration markers to prevent dehydration, a common trigger for SCD crisis, alongside pain management and emergency care. An easy-to-read booklet outlines key symptoms, medication schedules (including hydroxyurea and folic acid), potential side effects, and nearby free or low-cost screening locations. To maximize engagement, custom-designed lanyards hold emergency identification cards, mini pill holders for daily vitamins, and QR codes to SCD resources. The intervention also leverages a text-based micro-education system that delivers daily reminders for hydration and medication adherence, weekly educational messages about SCD, and monthly prompts to schedule screenings. These messages are designed for mobile phones and do not require internet access. Moreover, recurring “Sickle Cell Sundays” hosted at local churches and schools offer 10-minute educational activities led by trained youth ambassadors and community health workers. This layered approach not only increases awareness and access but also embeds long-term health habits into daily life, empowering individuals and families with culturally relevant, stigma-free tools to support SCD management.
Literature Review
Sickle cell disease (SCD) is a growing public health concern in the United States, affecting approximately 100,000 people per year and contributing to organ failure and various underlying health complications (Data and Statistics on Sickle Cell Disease, 2024). According to the Centers for Disease Control and Prevention (CDC), approximately 90% of individuals living with SCD in the United States identify as African American or Black (Data and Statistics on Sickle Cell Disease, 2024). An estimated one in 365 infants born to African American parents inherits SCD, while 1 in 13 inherits sickle cell trait (Data and Statistics on Sickle Cell Disease, 2024). Following African Americans, the Latinx community represents the second most affected racial group in terms of SCD prevalence.
Multiple social and environmental factors contribute to the rise of SCD in the United States. Individuals living in financially unstable communities often lack access to consistent care, which can exacerbate disease severity and complications (Loo et al., 2021). A lack of proper nutrition, more common in low-income communities, may further worsen the effects of SCD (Loo et al., 2021). Inadequate education regarding genetically inherited diseases may also increase the prevalence of SCD (Loo et al., 2021). Furthermore, poor communication between patients and healthcare providers can result in delayed treatment of critical complications, prolong recovery and worsen disease progression. Since SCD disproportionately affects the African American community, individuals may face systemic racism, leading to undertreatment. The lack of sufficient support services may contribute to social isolation, negatively impacting the community. These intersecting factors underscore the need for a targeted public health intervention. To address these challenges, a digital intervention utilizing SMS messaging is proposed to promote awareness, provide education about SCD, and connect individuals to accessible care.
Justification for the Target Population
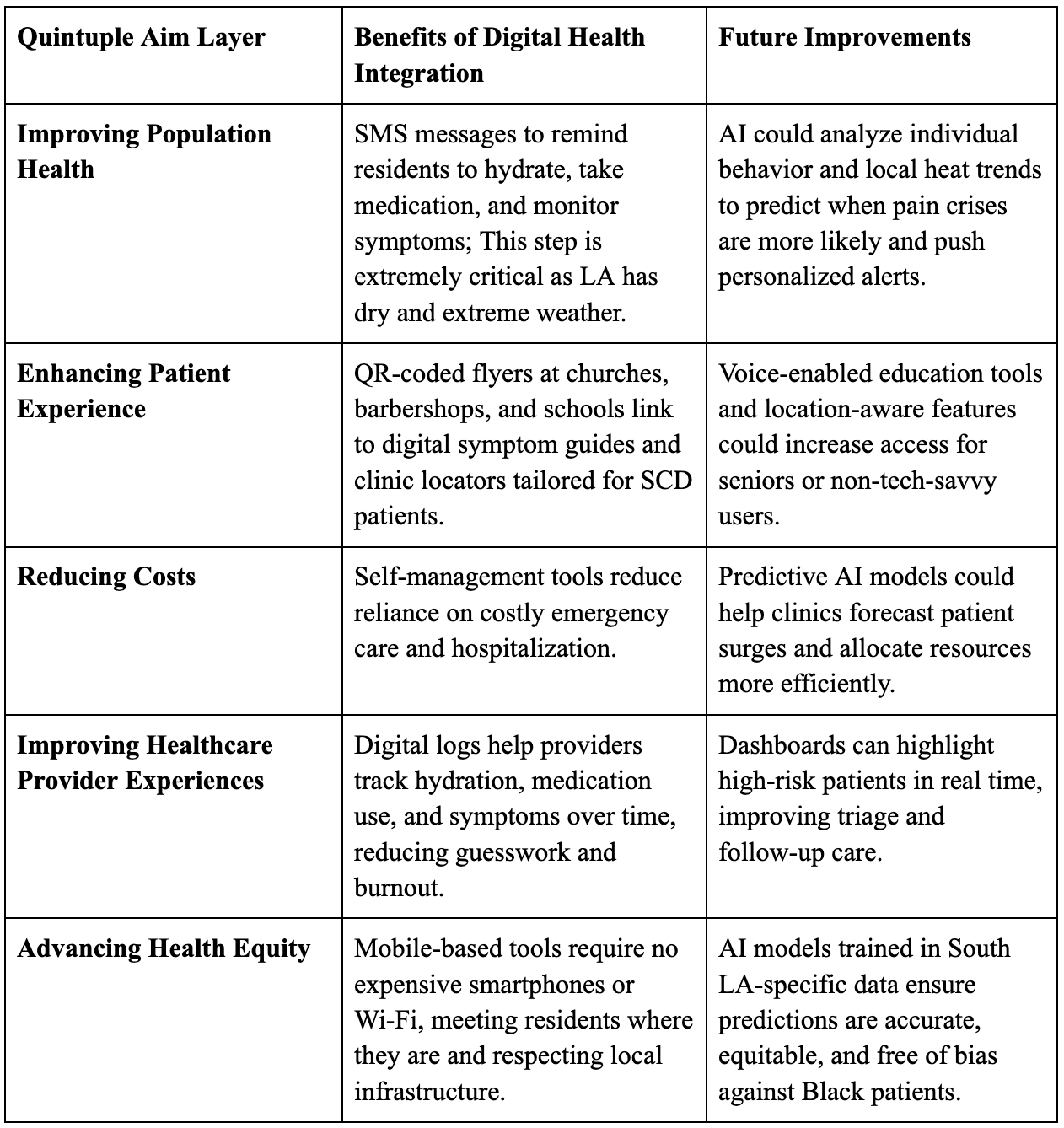
Table 1: Strategic Framework for Digital Health Integration and Future AI Enhancements within a Quintuple Aim Structure
Plan of Action
In areas such as View Park–Windsor Hills, a predominantly Black neighborhood in Los Angeles County, the burden of Sickle cell disease (SCD) is amplified due to limited access to specialized care and gaps in public awareness. Access to clinics, hospitals, and local medical infrastructure remains a challenge. SCD contributes to severe health complications, including chronic pain, organ damage, and frequent hospitalizations. Life expectancy for individuals with SCD is 20 years lower than that of the general population (Hematology.org, 2023). Despite advancements in treatment, including hydroxyurea (medication to reduce the need for blood transfusions) and gene therapy, the effectiveness of care in high-risk communities is often compromised by late diagnoses, transportation barriers, and more. Focusing on SCD in this community highlights the urgent need for targeted interventions to create sustainable, positive change.
Target population: African American residents of View Park–Windsor Hills, particularly adults aged 21 and older living with SCD or sickle cell trait. Outreach efforts prioritize underserved families and community hubs, including churches, schools, and employment centers, where access to SCD-specific education and care is limited.
Goals:
- Increase community awareness of SCD symptoms, risks, and preventative care strategies.
- Promote hydration, medication adherence, and timely recognition of crises.
- Establish a sustainable network of youth ambassadors, healthcare workers, and community partners to lead education and care initiatives.
Objectives:
- Launch 24 “Sickle Cell Sunday” events within 12 months, reaching at least 1,000 residents.
- Distribute 2,000 care kits (containing hydration bottles, symptom booklets, lanyards, and seasonal items such as electrolyte packets and hand warmers) to schools, clinics, and households.
- Implement an SMS alert system to provide weekly health tips and medication reminders.
Literature review and stakeholder perspectives:
SCD is a complex condition shaped by both biological and structural factors. These challenges are compounded by systemic inequities, which disproportionately affect underserved communities. To address these gaps, the intervention employs SMS messaging to promote awareness, deliver culturally relevant education about SCD inheritance, and connect individuals to resources such as nearby clinics and transportation assistance. This mobile-based approach ensures accessibility for communities with limited access to stable internet or in-person educational opportunities.
Stakeholder perspectives informed the intervention design. Input emphasized the importance of clear, transparent communication with families and fostering advocacy among future generations.
Intervention:
The program integrates mobile health tools, educational initiatives, and technology-driven outreach to address the unique needs of the View Park–Windsor Hills community. Specifically, biweekly Sickle Cell Sunday meetings will take place at local churches, providing informative sessions on hydration, environmental influences, and crisis management. Care packages containing water bottles with hourly markers, symptom checklists, and seasonal items such as electrolyte packets or hand warmers will be distributed. School-based workshops will be led by youth ambassadors to inform students and families about SCD genetics and early indicators. Additionally, a text messaging service will deliver weekly notifications on hydration, medication schedules, and extreme temperature alerts. Telehealth connections with hematologists at leading medical institutions, including UCLA Health and Children’s Hospital Los Angeles, will bolster these initiatives by supporting patients who require specialized care.
This approach aligns with program goals by increasing awareness, improving early identification of SCD symptoms, and promoting regular care practices through the integration of education, resource sharing, and technology. Implementation occurs in person through church gatherings, educational seminars, and workplace programs, as well as digitally through SMS alerts and online resources. Partnerships with local hospitals, faith-based organizations, schools, and nonprofit groups will foster trust and expand influence. Program effectiveness will be evaluated by analyzing event attendance, usage of care kits, pre- and post-surveys, and engagement metrics from the SMS platform.
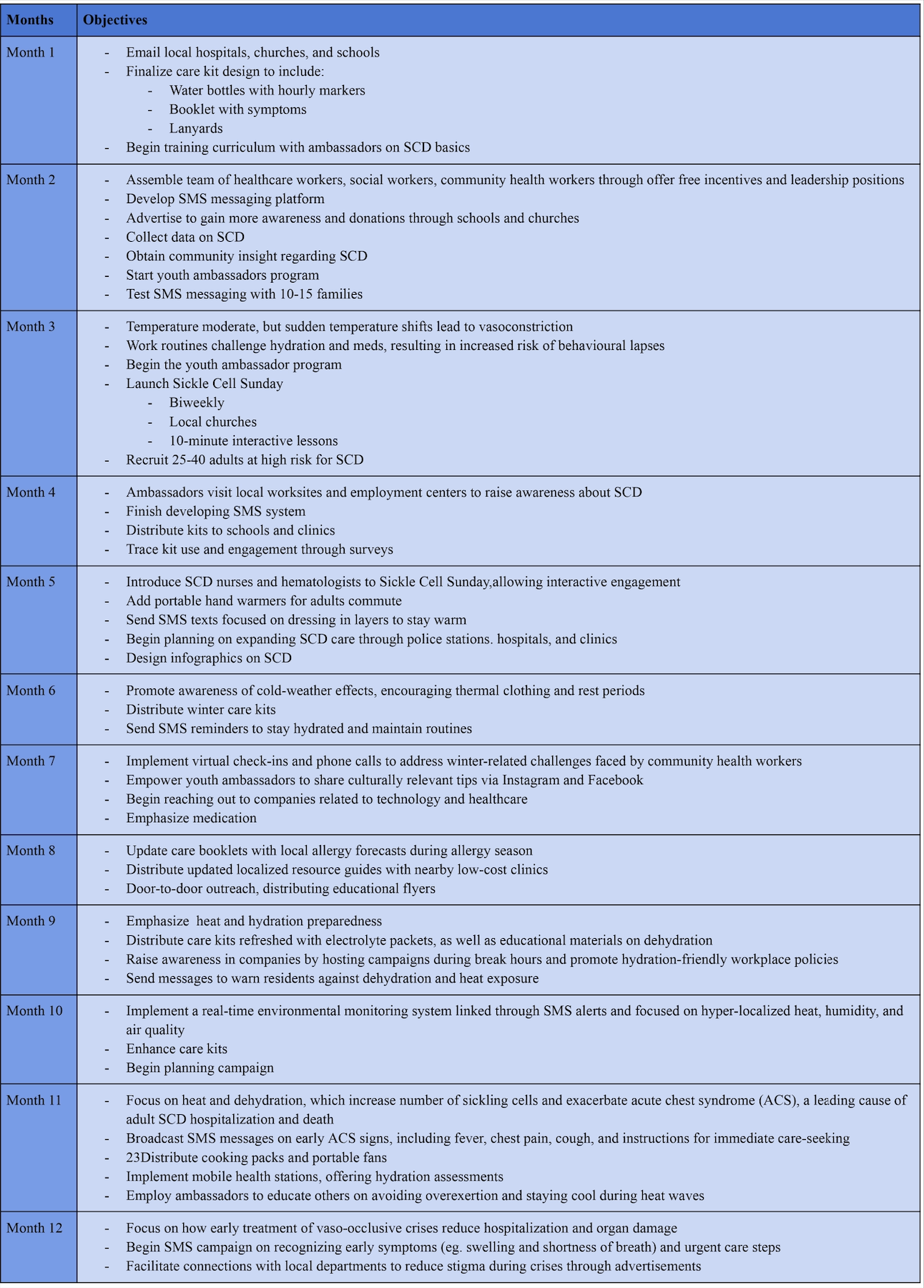
Table 2: Timeline and Strategic Objectives for the Initial Two-Month Implementation Phase of SCD Community Intervention
Essential materials include customized care kits equipped with hydration tools (hourly-marked water bottles, electrolyte packets), seasonal wellness items (handwarmers, fans), and educational booklets that explain SCD symptoms and triggers. Furthermore, the intervention invests in technology to develop an SMS platform to deliver real-time alerts and reminders for high-risk individuals. This platform will require initial setup costs and data tracking to ensure accurate and timely communication. Nurses, hematologists, social workers, community health workers, and youth ambassadors will be involved to conduct workshops, offer medical advice, and support outreach initiatives. Volunteers from nearby schools and churches may help with logistical tasks, including care kit distribution and event preparation. Training sessions will be conducted for youth ambassadors and church leaders to equip them with the knowledge and skills needed to provide accurate information regarding hydration, environmental factors, and crisis prevention. Partner churches, schools, and community centers will serve as event venues, reducing costs and leveraging established relationships with the community. Mobile health units, providing hydration evaluations and brief consultations, will require transportation, canopies, medical supplies, and temperature-monitoring equipment. Funding will be secured from multiple sources. Local healthcare institutions, including UCLA Health and the Martin Luther King Jr. Outpatient Center, have expressed interest in supporting outreach initiatives targeting underserved communities. These strategic partnerships are expected to provide not only financial support but also logistical support, clinical expertise, and access to educational materials.
The effectiveness of this intervention will be evaluated using a comprehensive, data-driven assessment approach. A combination of quantitative and qualitative methods will be employed to assess reach and impact. Primary indicators will include attendance at Sickle Cell Sunday events, total number of care kits distributed, and engagement metrics from the SMS platform (such as open rates, response rates, and click-through activity for health resources). Knowledge gains will be assessed through pre- and post-event surveys that measure participant understanding of hydration importance, symptom recognition during SCD crises, and awareness of local healthcare services.
Data collection will occur on a monthly basis to allow for timely program adjustments, while quarterly assessments will measure overall program progress. These quarterly evaluations will also incorporate community feedback meetings, thereby enabling local leaders, youth representatives, and participants to share their opinions on the quality, accessibility, and relevance of events. Collaborating with healthcare professionals from UCLA Health and Children’s Hospital of Los Angeles (CHLA) will allow for pattern recognition in hospital visits and emergency room admissions for SCD-related concerns to assess intervention effectiveness. To ensure long-term sustainability, church leaders and youth ambassadors will undergo official training as program facilitators, ensuring the ongoing success of both the SMS outreach and Sickle Cell Sunday events beyond the initial implementation period. An oversight committee will also be established, directed by the community and composed of healthcare experts, community leaders, and SCD supporters. This committee will meet biannually to review performance indicators, tackle issues, and strategize future improvements. This governance structure is designed to promote community accountability and ensure that the intervention remains responsive to evolving local needs and feedback.
Project UNITY
Project UNITY may improve the effectiveness of the intervention by serving as a strategic partner. Through UNITY’s established network of healthcare professionals, policy advocates, and public health experts, the program can receive guidance in developing a tailored training curriculum for youth ambassadors and community health advocates. UNITY may also facilitate connections with regional health leaders and policymakers, creating opportunities for a state-level initiative. Furthermore, UNITY’s mentorship and collaboration can strengthen partnerships with local hospitals, clinics, and nonprofit organizations. By leveraging UNITY’s expertise and network, the intervention has the potential to achieve immediate community-level impact and to be scaled across Los Angeles County and beyond.
Discussion
The intervention addresses key challenges faced by Black residents with SCD in View Park–Windsor Hills, California, by emphasizing prevention, education, and community-based support through engagement activities, an SMS texting system, and customized seasonal care kits. This approach aligns with the Quintuple Aim, which seeks to improve population health, enhance patient experience, reduce healthcare costs, support healthcare providers, and advance health equity. Sustainability is supported through integration into existing community infrastructure and continuous data collection via care kit utilization and SMS engagement. The program’s responsive design allows adaptation to seasonal and environmental changes, increasing both its relevance and long-term viability.
A major strength of the intervention approach is the customized care kit tailored to the specific needs of individuals with SCD, as SCD symptoms are often seasonally dependent. This intervention extends beyond reactive treatment by supplying patients with tools that mitigate environmental triggers, thereby reducing the frequency and severity of painful episodes before they occur. Additional strengths include the Sickle Cell Sundays program and the youth ambassador program, which are effective strategies to build knowledge, develop strong support systems, and empower community members to advocate for SCD awareness. The SMS alert system further enhances the intervention by delivering timely reminders based on environmental conditions such as heat, humidity, and air quality. The provision of free incentives and care resources represents another important strength. By reducing the financial burden, this intervention helps ensure access to essential prescriptions, therapies, and healthcare services.
Despite its strengths, the intervention faces potential challenges. Partnerships with local churches and schools cannot be guaranteed, which may limit program reach within the Windsor Park community. Additionally, survey-based evaluations may experience low response rates, increasing the risk of nonresponse bias. Insufficient or unrepresentative data could limit the ability to accurately assess program effectiveness and inform necessary adaptations over time. To address these limitations, supplemental data collection strategies, such as in-person surveys or random sampling methods, may be required to obtain more representative feedback. Another potential limitation is message fatigue associated with the SMS platform. If messages become overly frequent, their effectiveness may be reduced.
Conclusion
The prevalence of sickle cell disease (SCD) continues to rise nationwide, increasing by 41.4% from 2000 to 2021 (Dolai, 2024). With 90% of individuals living with SCD identifying as African American, targeted efforts are necessary to address systemic racism within the healthcare system and to ensure equitable, effective, and timely access to treatment. Expanding community-based programs beyond View Park–Windsor Hills to other predominantly African American communities nationwide has the potential to reduce disparities and amplify impact. Leveraging SMS messaging platforms allows critical health information to be delivered in an accessible, low-cost format, enabling individuals to better manage hydration, recognize symptoms, and seek care promptly. Future expansion efforts may include the use of social media campaigns to broaden outreach and increase visibility of SCD resources across diverse communities. Virtual programming, such as webinars and SMS messaging, could further extend support to individuals across multiple states. By prioritizing accessible education about SCD, such initiatives can highlight the healthcare needs of marginalized populations and strengthen advocacy efforts to improve SCD care and outcomes nationwide.
References
- National Institute on Drug Abuse. Addiction and Health. NIDA https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/addiction-health (2026).
- American Addiction Centers. Addiction Demographics: Which Socioeconomic Groups Struggle Most? American Addiction Centers https://americanaddictioncenters.org/rehab-guide/addiction-statistics-demographics (2026).
- Office of the Assistant Secretary for Planning and Evaluation. Affordable Care Act Expands Mental Health and Substance Use Disorder Benefits and Federal Parity Protections for 62 Million Americans. ASPE https://aspe.hhs.gov/reports/affordable-care-act-expands-mental-health-substance-use-disorder-benefits-federal-parity-protections-0 (2026).
- Andrilla, C. H. A., Patterson, D. G., Garberson, L. A., Coulthard, C. & Larson, E. H. Geographic variation in the supply of selected behavioral health providers. Am. J. Prev. Med. 54, S199–S207 (2018).
- Substance Abuse and Mental Health Services Administration. Behavioral Health Barometer: United States, Volume 6. SAMHSA https://www.samhsa.gov/data/report/behavioral-health-barometer-united-states-volume-6 (2026).
- Berwick, D. M., Nolan, T. W. & Whittington, J. The Triple Aim: Care, health, and cost. Health Aff. 27, 759–769 (2008).
- Nundy, S., Cooper, L. A. & Mate, K. S. The Quintuple Aim for health care improvement: A new imperative to advance health equity. JAMA 327, 521–522 (2022).
- Marmot, M. Social determinants of health inequalities. Lancet 365, 1099–1104 (2005).
- Compton, W. M., Thomas, Y. F., Stinson, F. S. & Grant, B. F. Prevalence, correlates, disability, and comorbidity of DSM-IV drug abuse and dependence in the United States. Arch. Gen. Psychiatry 64, 566–576 (2007).
- Compton, W. M. & Volkow, N. D. Major increases in opioid analgesic abuse in the United States: Concerns and strategies. Drug Alcohol Depend. 81, 103–107 (2006).
- Costello, E. J., Erkanli, A., Fairbank, J. A. & Angold, A. The prevalence of potentially traumatic events in childhood and adolescence. J. Trauma. Stress 15, 99–112 (2002).
- Allareddy, V. et al. Outcomes of acute chest syndrome in adult patients with sickle cell disease: predictors of mortality. PLoS ONE 9, e94387 (2014).
- American Society of Hematology. Longevity for those with sickle cell disease linked to care maintenance, family involvement. ASH https://www.hematology.org/newsroom/press-releases/2016/rare-patients-with-sickle-cell-disease-live-nearly-twice-as-long-as-average (2016).
- American Society of Hematology. Light-to-moderate exercise may bring benefits for sickle cell disease. ASH https://www.hematology.org/newsroom/press-releases/2019/light-moderate-exercise-may-bring-benefits-for-sickle-cell-disease (2019).
- Campbell, J. L. et al. Projecting Future Workload (NIHR Journals Library, 2019).
- Centers for Disease Control and Prevention. Data and statistics on sickle cell disease. CDC https://www.cdc.gov/sickle-cell/data/index.html (2024).
- Cholera, R. et al. Impaired cytoadherence of Plasmodium falciparum-infected erythrocytes containing sickle hemoglobin. Proc. Natl. Acad. Sci. USA 105, 991–996 (2008).
- Cleveland Clinic. Sickle cell crisis: symptoms, types & treatment. Cleveland Clinic https://my.clevelandclinic.org/health/diseases/sickle-cell-crisis (2024).
- AJMC. Improving outcomes for sickle cell disease by reducing health disparities. AJMC https://www.ajmc.com/view/improving-outcomes-for-sickle-cell-disease-by-reducing-health-disparities (2022).
- Centers for Disease Control and Prevention. Public health strategies for sickle cell disease. CDC https://www.cdc.gov/sickle-cell/initiatives/public-health-strategies.html (2025).
- HRSA. National sickle cell disease initiatives. HRSA https://www.hrsa.gov/sickle-cell-disease/national-initiatives/public-health-approach (2023).
- KFF. Sickle cell disease in the U.S.: an overview of racial disparities and policy issues. KFF https://www.kff.org/racial-equity-and-health/issue-brief/sickle-cell-disease-in-the-u-s-an-overview-of-racial-disparities-and-policy-issues/ (2024).
- Jordan, K., Phillips, S., Abrams, C. M. & Hall, G. Influence of social determinants of health across the lifespan for individuals with sickle cell disease. Health Promot. Pract. https://doi.org/10.1177/15248399251330215 (2025).
- Karkoska, K. A. et al. Academic challenges and school service utilization in children with sickle cell disease. J. Pediatr. 230, 182–190 (2021).
- Loo, S. et al. Addressing unmet basic needs for children with sickle cell disease in the United States: clinic and staff perspectives. BMC Health Serv. Res. 21, 50 (2021).
- Mangla, A. et al. Sickle Cell Anemia (Nursing) (StatPearls Publishing, 2023).
- McGlynn, M. C. et al. Education liaison improves implementation of school accommodations for students with sickle cell disease. Pediatr. Blood Cancer 70, e30602 (2023).
- Mayo Clinic. Sickle cell anemia. Mayo Clinic https://www.mayoclinic.org/diseases-conditions/sickle-cell-anemia/symptoms-causes/syc-20355876 (2025).
- MedlinePlus. Sickle cell disease. MedlinePlus https://medlineplus.gov/sicklecelldisease.html (2020).
- National Center for Education Statistics. Students with disabilities. NCES https://nces.ed.gov/programs/coe/indicator/cgg/students-with-disabilities (2024).
- National Heart, Lung, and Blood Institute. Sickle cell disease – causes and risk factors. NHLBI https://www.nhlbi.nih.gov/health/sickle-cell-disease/causes (2024).
- National Human Genome Research Institute. Sickle cell disease. Genome.gov https://www.genome.gov/genetics-glossary/Sickle-Cell-Disease (2019).
- UCLA Health. New UCLA Health sickle cell disease center aims to increase life expectancy for patients. UCLA Health https://www.uclahealth.org/news/article/new-ucla-health-sickle-cell-disease-center-aims-to-increase-life-expectancy-for-patients (2023).
- NHS. Causes – sickle cell disease. NHS https://www.nhs.uk/conditions/sickle-cell-disease/causes/ (2019).
- American Society of Hematology. Quantifying the life expectancy gap for people living with sickle cell disease. ASH http://hematology.org/newsroom/press-releases/2023/quantifying-the-life-expectancy-gap-for-people-living-with-sickle-cell-disease (2023).
- Schwartz, L. A., Radcliffe, J. & Barakat, L. P. Associates of school absenteeism in adolescents with sickle cell disease. Pediatr. Blood Cancer 52, 92–96 (2009).
- Shah, N. et al. Evaluation of vaso-occlusive crises in United States sickle cell disease patients: a retrospective claims-based study. J. Health Econ. Outcomes Res. 6, 106–117 (2019).
- WHO. Sickle cell disease. WHO | Regional Office for Africa https://www.afro.who.int/publications/sickle-cell-disease (2023).
- NORD. Sickle Cell Disease Foundation of California. RareDiseases.org https://rarediseases.org/organizations/sickle-cell-disease-foundation-of-california/ (2022).
- Sickle Cell Speaks. Sickle cell organizations. Sickle Cell Speaks https://www.sicklecellspeaks.com/support (2023).
- Su, E. et al. Humoral and cellular responses to mRNA-based COVID-19 booster vaccinations in patients with solid neoplasms under active treatment. ESMO Open 7, 100587 (2022).
- Children’s Hospital of Philadelphia. Supporting the Student with Sickle Cell Disease: A Comprehensive Handbook for Your School Community (CHOP, 2023).
- Kuznik, A. et al. Newborn screening and prophylactic interventions for sickle cell disease in 47 countries in sub-Saharan Africa: a cost-effectiveness analysis. BMC Health Serv. Res. 16, 304 (2016).
- Lee, L. et al. Reducing health care disparities in sickle cell disease: a review. Public Health Rep. 134, 599–605 (2019).
- Enabnit, A. et al. Vaso-occlusive crisis: understanding its causes, symptoms, management, and prevention. DoveMed https://www.dovemed.com/health-topics/focused-health-topics/vaso-occlusive-crisis-understanding-its-causes-symptoms-management-and-prevention (2023).
- Miller, A. C. & Gladwin, M. T. Pulmonary complications of sickle cell disease. Am. J. Respir. Crit. Care Med. 185, 1154–1165 (2012).
- Dolai, T. K. et al. Sickle cell prevalence in the universe problem in 2024. J. Hematol. Allied Sci. https://jhas-bsh.com/sickle-cell-prevalence-in-the-universe-problem-in-2024/ (2024).
Related Posts

Better Zoning Through Inter-city Cooperation
Figure: High Density Housing (Source: Geograph Britain and Ireland, Author:...
Read More
Addressing Medical Inequities in Healthcare Professional Deserts
This publication is in proud partnership with Project UNITY’s Catalyst Academy 2023...
Read More
Are We Driving Our Dogs Sick Through Our Urban Lifestyles?
Figure 1: Allergic disorders in humans and dogs are associated...
Read More
Preventing Peripheral Artery Disease in African Americans from Georgia: A Public Health Initiative
This publication is in proud partnership with Project UNITY’s Catalyst Academy 2024...
Read More
The Environmental Consequences of Civil Wars
Figure 1: This is the flag of Angola, the model...
Read More
Project Empathy: Addressing Substance Abuse in Low-Income Adolescents Across Baltimore
This publication is in proud partnership with Project UNITY’s Catalyst Academy 2024...
Read MoreDarius Dastur, Mishal Ali, Harshitha Ezhilarasan, Hasan Khan, Aaron Akasala