
This publication is produced in partnership with Project UNITY’s Catalyst Academy Class of 2025, a student public health research and education program.
Abstract
Alzheimer’s disease is a neurodegenerative condition characterized by progressive memory loss and cognitive impairment. While typically a medical diagnosis, Alzheimer’s disease also presents significant public health implications. This report aims to investigate both national and local prevalence of Alzheimer’s disease and dementia, and aims to explain how public health determinants can inform the development of a community-focused prevention in Baltimore. This report further aims to define how public health principles can be utilized to improve the quality of life for adults at risk for Alzheimer’s disease and dementia. A literature review was conducted using PubMed, JAMA network, and the National Institute of Health. A total of 39 peer-reviewed articles were reviewed and selected based on their credibility and relevance to the issue. Findings indicate that older adults, particularly Hispanic and Black populations in Baltimore, Maryland, are at higher risk for Alzheimer’s disease and related dementias compared to other racial and ethnic groups. Social determinants of health, including access to healthcare and economic stability, also influence risk, as limited income may contribute to risk factors such as an imbalanced diet, reduced physical activity, and limited access to dementia-related education. Based on these findings, a cost-effective public health prevention strategy was formulated to ensure accessibility for the target population.
Keywords: Alzheimer’s disease; dementia; Baltimore; socio-ecological model (SEM); social determinants of health
Introduction
Dementia refers to a group of neurodegenerative conditions characterized by progressive damage to neurons in the brain, leading to cognitive and motor function impairments and a reduced ability to live independently (Alzheimer’s Association, 2025). Alzheimer’s disease is the most common form of dementia. Because these conditions primarily affect people over 65, a population already considered vulnerable, targeted action is essential to support affected individuals and their families. Furthermore, the aging population in the United States continues to increase, and the number of dementia cases is expected to double by 2060 (Fang et al., 2025; Majoka & Schimming, 2021). To address this issue, organizations such as the Alzheimer’s Association provide educational programs and public resources to increase awareness of dementia risk factors and their role in the development of Alzheimer’s disease. These include non-modifiable risk factors, such as age and genetics, as well as modifiable risk factors, including poor nutrition, smoking, physical inactivity, social isolation, and limited cognitive engagement (Alzheimer’s Association, 2025). Social determinants of health, the conditions in which individuals are born, live, and work, play a critical role in shaping health outcomes and access to healthcare (Majoka & Schimming, 2021). These social determinants of health can also significantly influence the modifiable risk factors for Alzheimer’s disease and related dementia among older adults. For instance, lack of easy access to healthcare and economic instability can contribute to poor hygiene in impoverished areas, thereby increasing the overall health risk and, consequently, the risk of Alzheimer’s disease and dementia. Furthermore, risk factors such as smoking, alcohol consumption, and exposure to other chronic diseases? Diseases can cause damage to the brain that elevates the risk of these conditions.
Alzheimer’s disease and related dementia represent a major public health concern in the United States, specifically in cities and states of higher disease prevalence. With a high proportion of older adults, the city of Baltimore, Maryland, is one such region (Dhana et al., 2023). Addressing dementia in Baltimore has the potential to yield a significant positive impact on the city. With over 87,000 cases of dementia in Maryland currently, the government of Maryland has implemented initiatives aimed at reducing the prevalence of the disease. These efforts include the passage of the Dementia Services Act of 2022 and the establishment of specialized roles, such as the Director of Dementia Services Coordination (Maryland Department of Health, 2022). In addition, conducting comprehensive research and developing solutions in Baltimore can drive meaningful change at the grassroots level.
Public Health Lens
Alzheimer’s disease and dementia must be addressed through a public health framework as their growing prevalence indicates that addressing the issue at the individual level is insufficient. A public health approach is better for addressing this widespread issue because it emphasizes community health, overall well-being, and preventative measures. Given that Alzheimer’s disease currently has no cure, disease prevention remains the most effective means of reducing the number of individuals affected by this disease.Although certain drugs may slow disease progression, the primary focus still remains on lowering risk (Alzheimer’s Association, 2025).
A public health framework would also consider various non-medical factors, commonly referred to as social determinants of health (SDOH), which significantly contribute to disease risk. The five primary categories of SDOH include economic stability, education, social and community context, health and healthcare access, and neighborhood and built environment (US Department of Health and Human Services, 2020). These determinants are particularly relevant to Alzheimer’s, as it is considered a non-communicable disease. An approach integrating SDOH enables the development of more effective and sustainable interventions, working to reduce dementia prevalence.
The socio-ecological model (SEM) further enhances understanding of Alzheimer’s and dementia risk as this illustrates how factors across multiple levels (individual, interpersonal, institutional, community, and policy) interact to influence health outcomes (Golden & Earp, 2012). For example, diet is a key factor that influences risk of Alzheimer’s at the individual level (Alzheimer’s Association, 2025). While the Mediterranean diet is associated with reduced risk of Alzheimer’s and related dementia, diets high in fat, sodium, and cholesterol content are linked to increased risk. At the interpersonal level, social interaction is highly relevant, as active interactions with others have been shown to lower dementia risk (Alzheimer’s Association, 2025). At the organizational level, education initiatives at schools and workplaces—ranging from academic learning to fitness programs—can contribute to risk reduction. Community-level interventions, including awareness campaigns, are highly beneficial because increased awareness can promote healthy habits and the modification of risk factors. Finally, at the policy level, state legislation in Maryland has demonstrated a commitment to addressing Alzheimer’s disease and related dementia through laws. (Maryland Department of Health, 2022).
Methods
Data on Alzheimer’s disease and dementia were retrieved from multiple databases, including Google Scholar, PubMed, the National Institute of Health, and the JAMA Network. Articles were included if they were published within the last 25 years, contained relevant and detailed information, and were available in full-text format at no cost. In total, 39 articles that met the inclusion criteria were reviewed and analyzed. Stakeholder interviews were conducted to gain contextual insights. Stakeholders were selected based on their expertise, relevance to the chosen city, and a review of their prior efforts aimed at addressing Alzheimer’s disease and related dementia. Based on the findings from the literature review and stakeholder input, an evidence-based plan of action was developed after synthesizing and extrapolating key findings from the literature review.
Literature Review
Alzheimer’s disease and related dementia are a growing public health concern in the United States, affecting approximately seven million people annually (Alzheimer’s Association, 2025). These conditions not only contribute substantially to increased healthcare costs but also place significant burdens, like stress and anxiety on financial costs, on millions of families. It is estimated that by 2060, 13 million adults over the age of 65 will be living withAlzheimer’s disease or related dementias (Fang et al., 2025; Majoka & Schimming, 2021).
An epidemiological study conducted across all 50 U.S states indicates that specific demographics, such as age, sex, race and ethnicity, and educational attainment, are key determinants of risk for Alzheimer’s disease and dementia (Dhana et al., 2023). For example, among adults aged 65 and older, approximately one in nine is affected by Alzheimer’s or dementia. Furthermore, 74% reported cases across the U.S. occur among individuals aged 75 or older (Dhana et al., 2023), suggesting a strong association between increasing age and disease prevalence. In terms of sex, females over 65 have historically exhibited a higher risk of Alzheimer’s disease compared to men, although this disparity has narrowed in recent years. Persistent inequalities in education, income, and racial and ethnic groups further contribute to disease prevalence. As such, Black and Hispanic older adults are disproportionately affected compared to non-Hispanic White populations (Alzheimer’s Association, 2025; Hudomiet et al., 2022). Notably, Blacks individuals with first-degree relatives diagnosed with Alzheimer’s disease were more likely to develop the condition themselves than their White counterparts with similar family histories (Hudomiet et al., 2022). Despite how genetic predisposition increases susceptibility, disease development is not guaranteed. Thus, 35 to 40% of dementia cases are attributable to modifiable risk factors, underscoring the importance of proper prevention strategies (Rolandi et al., 2020).
Social determinants of health (SDOH) play a significant role in Alzheimer’s and Dementia, particularly factors including economic stability, educational access and quality, and healthcare access and quality (Llibre‐Guerra et al., 2024). According to the Alzheimer’s Association, lower socioeconomic status is associated with an increased chance of developing Alzheimer’s disease and dementia. Low income is associated with faster cognitive decline (Majoka & Schimming, 2021). Poverty also contributes to disease risk through mechanisms including food insecurity and inability to afford healthcare insurance.
Because brain health is closely linked to cardiovascular health, determinants such as diet and lifestyle can have a profound effect on one’s likelihood of being diagnosed with Alzheimer’s and Dementia. Poor diet or physical inactivity, which proves to increase cardiovascular disease risk, also in turn elevates the likelihood of developing Alzheimer’s disease and dementia (Alzheimer’s Association, 2025). Additionally, smoking has been identified as a significant contributor, with approximately 14% of global dementia cases attributed to tobacco use (World Health Organization, 2014). Limited access to proper healthcare can increase stress and anxiety, further exacerbating cognitive outcomes. Educational attainment is another critical determinant; lower education levels are associated with an increased rate of dementia (Majoka & Schimming, 2021), whereas a more rigorous education may work to strengthen cognitive abilities such as memory, critical thinking, and reasoning, and reduce/delay? symptom onset. Employment type also influences risk. Occupations requiring less intellectual engagement and intensity are associated with higher rates of Alzheimer’s disease and dementia (Majoka & Schimming, 2021). Finally, social and community context play a crucial role. For example, reduced social engagement has been linked to cognitive decline and an increased dementia risk (Majoka & Schimming, 2021).
Justification for the Target Population
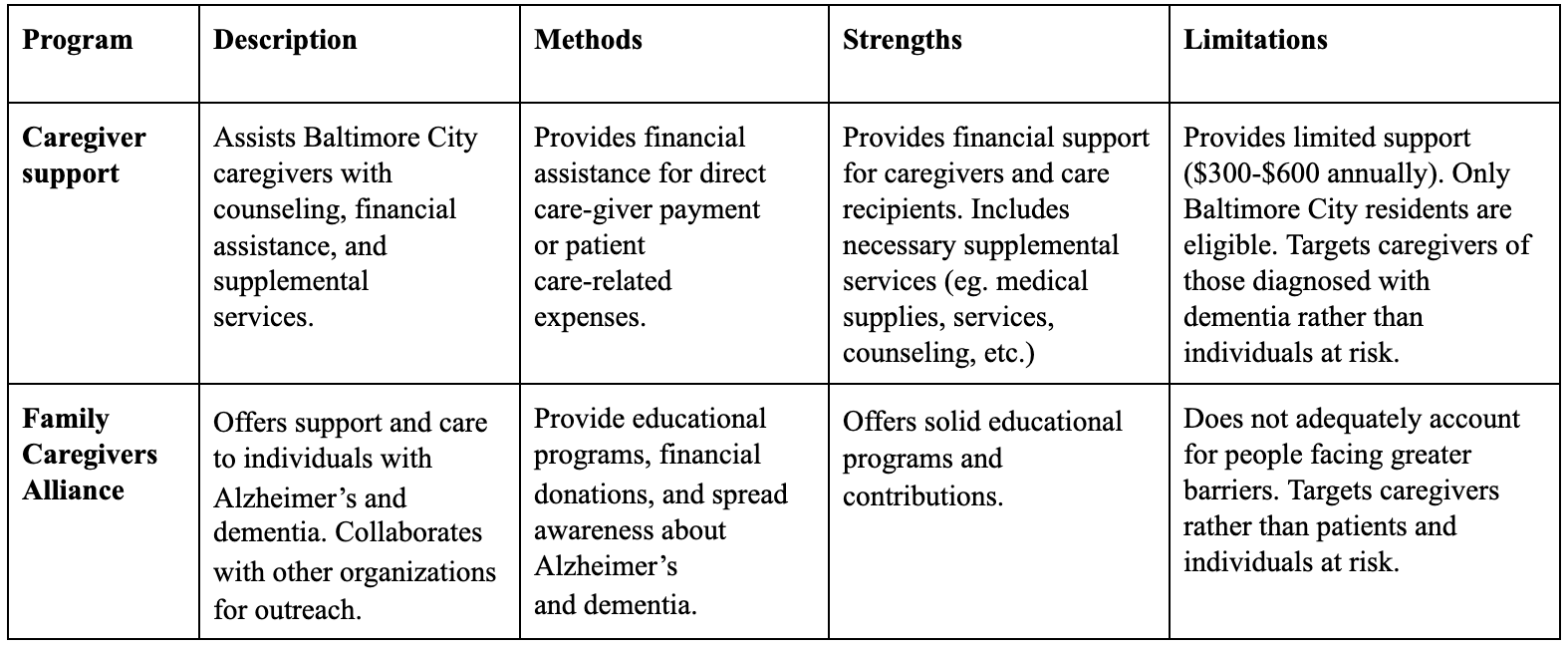
Table 1: Existing Interventions
Existing Interventions
Digital health solutions integrate digital technology to create solutions for addressing health-related issues. These solutions include the use of mobile apps and artificial intelligence, among other technologies, thereby increasing accessibility and efficiency through reaching large numbers of people quickly (Abernethy et al., 2022). For Alzheimer’s and dementia, digital health solutions can be particularly useful for raising awareness and delivering education. Although a variety of digital platforms are available, web-based platforms may be the most familiar and accessible option for individuals over the age of 50.
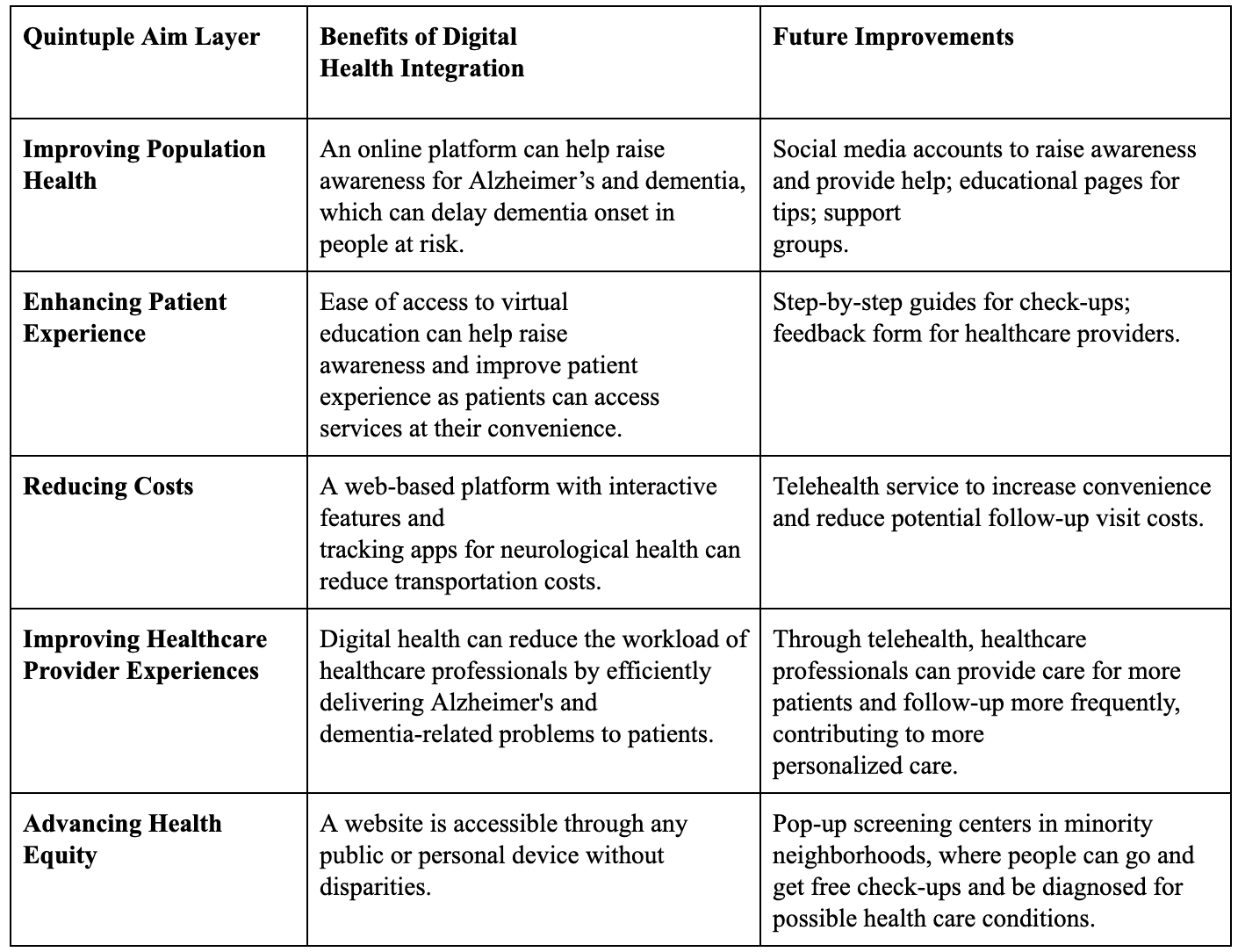
Table 2: Quintuple Aim of Healthcare
Plan of Action
This intervention and prevention program aims to support individuals over the age of 50 residing in Baltimore, Maryland who are at high risk of disease, particularly African-American and Hispanic populations. We plan to create a user-friendly website, Balto-Mind, that combines both existing and new resources for those at risk for Alzheimer’s and a$llows users to make donations to charitable organizations directly through our platform. Our objectives are to reach 100,000 website views within six months and generate at least $200 dollars in donations.
Specifically, Balto-Mind will feature five main components: (1) Education section with links to the Alzheimer’s Association and Maryland Department of Health. This section will also include self-assessments, interactive components, and an AI chatbot to provide answers and resources for individuals and support systems. (2) Clickable links to donation sites. (3) Section with guidance on diet and exercise, including nutrition details, trivia games, and sample diet plans. (4) Resources and links to prevent smoking. (5) Section for improving cognition and social engagement. There will be links to activities such as puzzles, Sudoku, and word searches to enhance cognitive function, as well as up-to-date information about community groups and social activities, including book clubs.
Local stakeholders in Baltimore, Maryland, including primary care offices, neurology clinics, and nursing homes, will assist with implementing this intervention publicly. Visitors to the website will be a comprehensive compilation of resources that they may not have encountered elsewhere. All services are free, making the platform easily accessible and more appealing to individuals and their families. Increased web traffic will likely increase donation rates over time.
To gain insight of the impact on the community, the effectiveness of this intervention will be evaluated monthly by tracking web traffic and soliciting feedback through a survey. Additional tools, such as polls and traffic meters will be helpful in further assessing user satisfaction. Monitoring donations and engagement will be useful in enhancing the website.
Developing the website will require key resources, including, including the domain,, website development software, and potential tools like a SAGE screening tool or video conferencing app to enhance user experience. Funding and support may come from stakeholders or clinics in the Baltimore area, and the team at Project UNITY may additionally utilize their experience to establish strong ties with local initiatives and promote the website.
Timeline:
Month 1:
- Website development (Include resources for dementia patients and their families (ex. What to do and who to talk to, sage, etc.)
Month 2:
- Testing period (Invite local professionals and clinics to review website features)
Month 3:
- Market the website (Through Instagram and in person, including a description of goals and FAQ)
Month 4:
- Create an AI chatbot that allows people to provide feedback on the website
Month 5:
- Maintenance period (Review feedback and incorporate fixes or new implementations)
Month 6:
- Continue marketing and touching up the website
Month 7:
- Make a donation link
Month 8:
- Track donations and website traffic
Month 9:
- Advertise monthly trainings and support meetings
- Outreach to more clinics
Month 10:
- Continue tracking website traffic and user feedback.
- Make improvements
Month 11:
- Hold virtual trainings and support meetings on the 2nd Thursday of each month
- Ensure the website is easily accessible from all devices
Month 12:
- Follow up with stakeholders and leaders in the field to gain insight on their impression of our implementation
Strengths and Limitations
A website is one of the most streamlined approaches for engaging individuals, regardless of location, to support the local community. It allows for easy compilation of various resources, ensuring accessibility for users. For populations over the age of 50, websites are generally easier to navigate than other digital platforms, such as mobile apps.Another key strength is community support. The website provides value through offering information to individuals at high risk for Alzheimer’s and dementia, as well as their caregivers and loved ones, thereby providing assistance.
While there are strengths, there are also limitations. Technical challenges, such as website compatibility issues with browsers, disrupted performance on mobile devices, and potential security breaches, are possible. Additionally, with other websites covering similar topics, ensuring that users discover this website may prove to be a challenge. Potential solutions include monthly monitoring for malfunctions and security issues, along with timely fixes. Another limitation is that some individuals in underserved communities may lack access to a device. This issue could be addressed through government funding to provide electronic devices and internet access in these affected areas.
Discussion and Conclusion
Research has shown that the city of Baltimore has among the highest rates of Alzheimer’s disease and related dementias nationally, a disease that is characterized by memory loss and overall cognitive decline among the elderly. In Maryland, there are currently over 87,000 cases in Baltimore alone. In particular, Black and Hispanic seniors in Baltimore, the target population, have a greater chance of developing the disease compared to the White population. Research deduces that this is most likely due to factors such as the average socioeconomic status of these ethnic groups, as well as factors such as diet.
A public health perspective allows understanding the high risk of Alzheimer’s disease and related dementias for Blacks and Hispanics in Baltimore from the perspective of health equity, where these minority groups may not have access to education, resources, and adequate health care needed that may protect them against the risk of Alzheimer’s disease and related dementias Since Alzheimer’s disease and related dementias do not have a cure, professionals from multiple fields should collaborate to execute preventative measures (ie, awareness campaigns, websites, etc) to address it through a multidisciplinary approach, so that they can expand the range of people they can assist and facilitate the combination of expertise to foster better innovation. Therefore, it is extremely important to design solutions, such as developing accompanying mobile apps to improve accessibility for individuals who have mobile devices, that are mindful of the digital health shift and the Quintuple Aim, as the world is becoming increasingly digital. The website will thus feature engaging visuals to inform users about Alzheimer’s disease and related dementias in Baltimore and throughout larger cities and international populations, and donations go directly to organizations, including the Alzheimer’s Association of Greater Maryland. This intervention can also act as a preventative measure for those who do not have Alzheimer’s disease and related dementias, as the website will contain numerous resources that can be useful for caregivers seeking information on how to prevent this disease in their loved ones. This would help expand the reach and impact of the intervention.
References
- Abernethy, A. et al. The promise of digital health: then, now, and the future. NAM Perspect. 2022, 10-31478 (2022).
- Alzheimer’s Association. Alzheimer’s Disease Facts and Figures (Alzheimer’s Association, 2025).
- Boyle, P. A. et al. Attributable risk of Alzheimer’s dementia attributed to age-related neuropathologies. Ann. Neurol. 85, 114–124 (2019).
- Dhana, K. et al. Prevalence of Alzheimer’s dementia in the 50 US states and 3142 counties. Alzheimers Dement. 19, e074430 (2023).
- Fang, M. et al. Lifetime risk and projected burden of dementia. Nat. Med. 31, 772–776 (2025).
- Golland, Y., Ben-David, B. M., Mather, M. & Keisari, S. Playful brains: a possible neurobiological pathway to cognitive health in aging. Front. Hum. Neurosci. 19, 1490864 (2025).
- Golden, S. D. & Earp, J. A. L. Social ecological approaches to individuals and their contexts. Health Educ. Behav. 39, 364–372 (2012).
- Hudomiet, P., Hurd, M. D. & Rohwedder, S. Trends in inequalities in the prevalence of dementia in the United States. Proc. Natl Acad. Sci. USA 119, e2212205119 (2022).
- Llibre-Guerra, J. J. et al. Social determinants of health but not global genetic ancestry predict dementia prevalence in Latin America. Alzheimer’s Dement. 20, 4828–4840 (2024).
- Lines, L. M. & Wiener, J. M. Racial and ethnic disparities in Alzheimer’s disease: a literature review (U.S. Dept. of Health & Human Services, 2014).
- Majoka, M. A. & Schimming, C. Effect of social determinants of health on cognition and risk of Alzheimer disease. Clin. Ther. 43, 922–929 (2021).
- Maryland Department of Aging. Brain Health (Maryland Dept. of Aging, 2025).
- Maryland Department of Health. Maryland State Plan to Address Alzheimer’s Disease and Related Dementias: 2022–2026 (Maryland Dept. of Health, 2022).
- National Institute on Aging. MIND and Mediterranean diets linked to fewer signs of Alzheimer’s brain pathology (NIA, 2023).
- Pillai, J. A. et al. Association of crossword puzzle participation with memory decline. J. Int. Neuropsychol. Soc. 17, 1006–1013 (2011).
- Qiu, C., Kivipelto, M. & von Strauss, E. Epidemiology of Alzheimer’s disease. Dialogues Clin. Neurosci. 11, 111–128 (2009).
- Rolandi, E. et al. Estimating the potential for dementia prevention through modifiable risk factors. Alzheimers Res. Ther. 12, 94 (2020).
- Sharp, E. S. & Gatz, M. Relationship between education and dementia. Alzheimer Dis. Assoc. Disord. 25, 289–304 (2011).
- Treadwell, K. How a Baltimore city initiative improves healthcare equity. The Black and White (8 Feb 2025).
- U.S. Department of Health and Human Services. Healthy People 2030 (HHS, 2020).
- World Health Organization. Tobacco and Dementia (WHO, 2014).
Related Posts

M.A.M.A: Mobilizing Activism for Maternal Access in Clifton, Ohio
This publication is produced in partnership with Project UNITY’s Catalyst...
Read More
Trust: The Essence of Good Policy Implementation
Figure 1 President Tsai Ing-wen inspects the Central Epidemic Command...
Read More
The Growing Prevalence of Anxiety as a Public Health Issue
This publication is in proud partnership with Project UNITY’s Catalyst Academy...
Read More
A Novel Mental Health Literacy Education Program for Pre-Teens
Figure: A typical elementary school classroom in Japan (Cassidy, 2005). Source:...
Read More
The Public Health Humanitarian Crisis in Ukraine
This publication is in proud partnership with Project UNITY’s Catalyst Academy 2023...
Read More
The Public Health Crisis of Alzheimer’s Disease in African American and Hispanic Populations
This publication is in proud partnership with Project UNITY’s Catalyst...
Read MoreDarius Dastur, Mishal Ali, Harshitha Ezhilarasan, Hasan Khan, Aaron Akasala