
This publication is produced in partnership with Project UNITY’s Catalyst Academy Class of 2025, a student public health research and education program.

Abstract
Inflammatory Bowel Disease (IBD), including Crohn’s disease and ulcerative colitis, affects an estimated 2.4 to 3.1 million people in the US, with healthcare costs around $8.5 billion in 2018.4 The disease is rising in prominence in many urban areas (such as Chicago),14 and its prevalence is currently highest in non-Hispanic White populations, though increasing in African American, Hispanic, and Asian groups as well.3 IBD causes chronic pain, nutritional deficiencies, and a lower quality of life; currently, it is treated through immunosuppressants (ISx).1 Due to these factors, we are investigating the prevalence of IBD in Chicago, its social determinants of health, and how public health professionals can respond. We conducted our research primarily from PubMed, through which we used 22 articles total. Additionally, we conducted interviews with stakeholders to gain a deeper understanding of IBD and recent advances in its treatment. Focusing on Chicago, some of the largest populations at risk are Black and Hispanic communities.9,5,13 Local and national data reflect that these groups face higher complications due to healthcare access disparities and socioeconomic barriers.19 The social determinants of health are insurance gaps, food insecurity, and healthcare access disparities, which worsen health outcomes for at-risk populations. Overall, our findings of the significant treatment gaps for IBD treatment apply nationwide. These require impactful public health initiatives to address the root causes of treatment gaps.
Keywords: Inflammatory bowel disease; IBD; Crohn’s disease; ulcerative colitis; health disparities; urban health; public health; diet
Introduction
Inflammatory Bowel Disease (IBD) is a chronic autoimmune disorder characterized by inflammation and irritation of the gastrointestinal tract. Worldwide, the prevalence of the disease remains at 0.3%.15 While seemingly low, the chronic nature of the disease, lifetime treatment costs, and quality of life impacts make it a significant issue. The condition diverges into two primary states: one is ulcerative colitis (UC), and the other is Crohn’s disease (CD). Both are crucial health concerns within the US; as of 2019, the US Age-Standardized Incident Rate (ASIR) for IBD was 4.5 times higher than global averages.11 This is a pertinent issue in Chicago, Illinois, as genetic predisposition, environmental factors, and limited healthcare access contribute to the local average of 117 cases per 100,000 people.7 If this issue is not addressed, thousands of individuals will live with untreated abdominal pain that will remain forever untreated, due to the misconception of being a simple stomach ache. Despite these warning signs, healthcare costs are still high, with the average annual cost for treating ulcerative colitis and Crohn’s disease being $5,066 and $8,265, respectively.12 Within this report, our team analyzed the potential side effects that result from the use of ISx to treat IBD patients by utilizing a multi-step intervention that will address IBD in the high-risk population of Chicago; this will then be further expanded to a national scale. The literature review will provide more details about IBD and its prevalence, while the methods will talk about how the research was conducted as well as stakeholder perspectives. Following this, our step-by-step plan for intervention is provided in detail; the public health lens and digital health solutions offer more information on various ways our intervention can be applied and show different solutions to help with IBD. Finally, the discussion and conclusion will review our intervention and its usage as well as evaluate potential future research.
The Importance of a Public Health Lens
Across the United States, the prevalence of inflammatory bowel disease is rising, with significant variations in health behaviors. Compared to adults without IBD, these variances included the practice of smoking (21% vs. 26%), sleeping for less than seven hours a day (32% vs. 38%), and decreasing beneficial aerobic muscle activity (45% vs. 50%).4 Further growth in the prevalence of the disease may be attributed to the country’s aging population, with the highest prevalence of the disease occurring among individuals aged 45 and above.4 As this condition continues to increase in Americans, so does the cost of IBD healthcare. A recent study conducted in 2018 estimated that the overall cost of IBD-related care amounted to $8.5 billion, highlighting IBD’s influence on US families and individuals.4
The socio-ecological model reveals the deeper health disparity beyond the clinical diagnosis of IBD by considering multiple levels of influence on a patient’s outcome.4 The socio-ecological model was used to analyze the relationships between individuals and their environment at 4 main levels, which will also be further elaborated on in the literature review. Starting with the individual level, biological and behavioral factors can affect the prevalence of IBD.1 Secondly, the interpersonal level also significantly impacts cases of IBD by straining relationships over time.1 Having a strong family and peer support system can help patients deal with symptoms and feel accepted while facing a disease. Third, at the community level, access to healthcare can also significantly impact patient outcomes from IBD.8 Patients in rural or underserved areas may face more challenges seeking a gastroenterologist and treating their condition, potentially leading to it going unresolved. Fourth, at the organizational level, healthcare systems and their quality can play a large role in how IBD patients receive care – an overburdened healthcare system can lead to delays in diagnosis and treatment.19 Finally, at the societal level, socioeconomic status can play a significant role in determining whether patients have access to treatment or education.9 Overall, the socio-ecological model showcases the disparities and trials that individuals with IBD undergo, and why this analysis is critical to understanding how to best treat these individuals.
Methods
We extracted our data from PubMed, as it is an extensive and informative database that contains many publications relating to Inflammatory Bowel Disease, and the side effects of ISx in combating it. We decided not to read into articles that came from opinionated and unverifiable sources. We also avoided using articles that were dated before 2008, as the information in these articles could be outdated. In total, we read 22 articles for our research paper. We performed our stakeholder interviews by looking for professors working at Chicago universities who specialize in IBD. This process allowed us to interview a professor specializing in Crohn’s disease at Northwestern University. In our fruitful discussion, we discussed the history of IBD, current treatment, and what researchers are doing in the future. We designed our plan of action by learning from Chicago residents with IBD and listening to their concerns.
Literature Review
Inflammatory Bowel Disease, or IBD, is a chronic immune-mediated disorder that primarily affects the gastrointestinal tract. It encompasses ulcerative colitis (UC) and Crohn’s disease (CD).14 Immunosuppressive drugs (ISx) have been growing in popularity in their usage to fight IBD. However, specific medications, such as 6-MP/AZA, have led to serious side effects such as hepatitis, pneumonitis, arthritis, fever, and pancreatitis. Treatments for IBD include immunomodulatory drugs such as methotrexate, cyclosporine, and other biologics, and immunosuppressive drugs (ISx). However, these treatments have been linked to serious side effects such as hepatitis, pancreatitis, and an increased risk of infection.20 Other than immunosuppressive therapy, other treatments include immunomodulatory therapies, including methotrexate, cyclosporine, and biologics.20 Furthermore, ISx has also been associated with increased infection risk, along with reemergence of latent tuberculosis, suggesting the need for careful monitoring of patients treated with ISx.8
A risk that occurs with immunosuppressive therapy in the use of IBD is the increased probability of infections and cancers. Because these treatments dampen the immune system’s response to potential infections (which is to act to reduce inflammation), certain pathogens can be left undetected, meaning they can spread easily. Nonetheless, the implementation of mucosal healing balances these side effects, reducing the risks of illnesses stemming from intestinal lesions, malnutrition, and IBD-related surgeries. Treatments such as corticosteroids increase the prevalence of vascular thromboembolic events; however, this may be counteracted through other immunosuppressive drugs that allow deep remission from IBD symptoms. These risks also vary based on patient age and sex. Accordingly, while tumor necrosis factor antagonists increase infection risks in all ages, thiopurines only impact young patients.2 Therefore, it is of the utmost importance to consider the patient’s age, background, and clinical history when determining the risks of immunosuppressive therapy.
Our research team consists of members from Chicago, Philadelphia, and Arkansas, and data reports disproportionately find that Chicago is most affected by IBD. This is largely due to Chicago’s racial inequality and historic economic segregation. Data from the Illinois Department of Public Health has reported disproportionate IBD burdens among African American and Hispanic populations in the cities, with disparities in the prevalence of the disease, its treatment, and health outcomes.7 In Illinois, around 1.5% of adults have IBD, with neighborhoods in Chicago such as Englewood, Austin, and West Garfield Park experiencing higher hospitalization rates compared to the state average.7 Black and Hispanic adults aged 24-45 are more likely to be hospitalized due to IBD, with hospitalization rates 30-40% higher than those of other demographic groups.
On the individual level, factors such as genetics, diet, stress, and financial status significantly improve the likelihood of developing IBD. This is because eating processed foods has been linked to an increase in flare-ups, a diet that lower-income patients are more likely to fall victim to due to food deserts, rising costs of fresh food, and systemic inequities in nutrition. Financial status is also a significant factor, as cost-related medication noncompliance affects 25% of Chicago residents, limiting the effectiveness of ISx.5 Lower-income residents are also more likely to develop chronic diseases due to food insecurity.19
Moving to the interpersonal level, the presence of a strong family and social support makes it much easier for patients to manage their IBD and seek effective treatment. However, stigma within some communities in Chicago also makes it difficult to seek treatment, reducing medication adherence.11
At the organizational level, schools with limited health accommodations can increase stress and make it more likely for students to skip classes, also making it less likely that they will reach out for help. This can hurt their education and make them less likely to seek help for IBD flare-ups.7 Interestingly, there is no research ongoing to investigate inequities in the treatment of IBD patients with learning disabilities.10
At the community level, many people do not have access to support groups based on their socioeconomic status. This makes it harder to find others with their condition and seek help, reducing the likelihood of people seeking treatment.
Finally, policy-level factors such as the expansion of Medicaid in Illinois have improved treatment outcomes and made it easier for those with IBD to seek therapy. However, this has yet to cover all affected groups, such as undocumented residents. Further policies promoting health literacy in multiple languages will help more people, regardless of their background, get the treatment they deserve.21
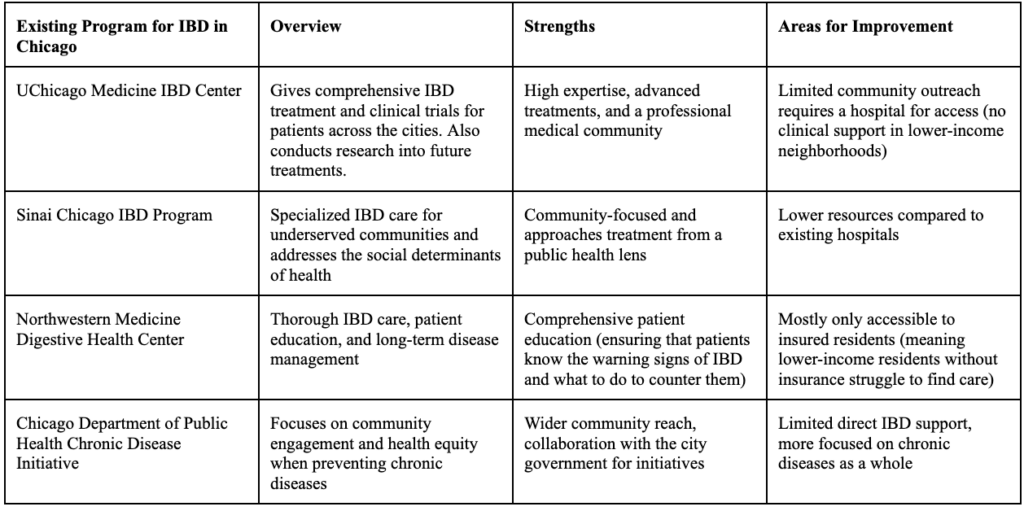
Table 1: Overview of IBD Programs for Marginalized Communities in Chicago
The Quintuple Aim model is a five-pronged approach to enhancing the patient experience and fostering trust, communication, and engagement between patients and physicians.13 It provides a comprehensive roadmap for improving patient care by focusing on five main goals:
- Improving Population Health
- Enhancing Patient Experience
- Reducing Costs
- Improving Healthcare Providers’ Experiences
- Advancing Health Equity
When applying the Quintuple Aim model to IBD, public health experts can deliver a more holistic and sustainable approach to controlling the disease. Since IBD is a chronic condition that requires coordinated care across multiple medical specialties, proper communication and coordination are necessary for improving patient outcomes. We will now explore the individual sections of the Quintuple Aim model in more detail:
- Improving Population Health – the goal is to reduce the overall incidence of IBD in the target population (underserved communities in Chicago). This can be achieved by screening high-risk groups (e.g., individuals with a family history of the disease or those belonging to certain ethnicities with a higher risk of developing the condition) to detect signs of the disease early.
- Enhancing the Patient Experience – the goal is to deliver personalized and effective care to patients with IBD. In combating this disease, this goal will provide individualized treatment plans, improve access to gastroenterologists, and ensure that patients receive adequate education about medications and lifestyle.
- Reducing Costs – the goal is to lower overall healthcare costs while also maintaining quality for IBD treatment. In this specific case, there should be a switch from reactive to proactive preventive care to improve diagnosis and treatment outcomes. Furthermore, using telehealth for virtual check-ins will provide a faster and safer method for diagnosis.
- Improving Healthcare Providers’ Experiences – the goal is to reduce provider burnout and improve job satisfaction. This can be achieved by supporting gastroenterologists, nurses, and/or psychologists, reducing administrative burdens like excessive documentation and charting, and ensuring that physicians have adequate days off to improve mental health and motivation.
- Advancing Health Equity – the goal is to reduce disparities in healthcare access. In combating IBD, addressing barriers faced by underserved populations, developing culturally sensitive care (such as brochures about ISx in multiple languages or online videos in other languages about the treatment), and ensuring equitable access to diagnostics, treatments, and insurance coverage can be ways to promote health equity.
There has been a large shift towards digital technology in improving public health, especially in IBD. For example, telemedicine has been used more and more frequently in treating IBD – something that could be expanded more in the future.9 With IBD cases rising, many systems now use remote monitoring and AI to offer care. These tools have helped doctors track health symptoms and signs in these patients to maintain their health. There have also been new ways that IBD education has been spread, such as social media events and other digital platforms.
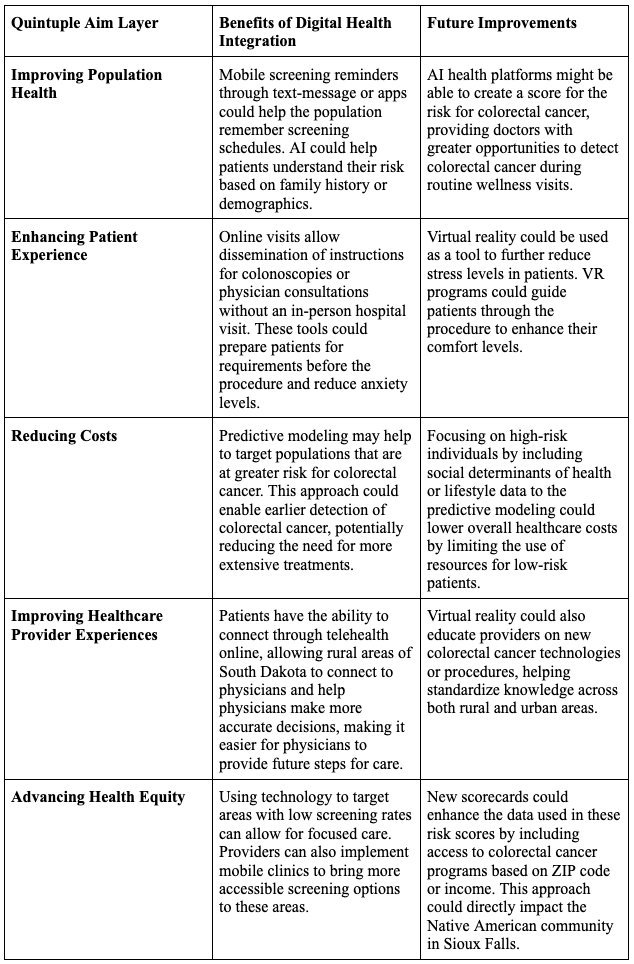
Table 2: Overview of Quintuple Aim Model
Plan of Action
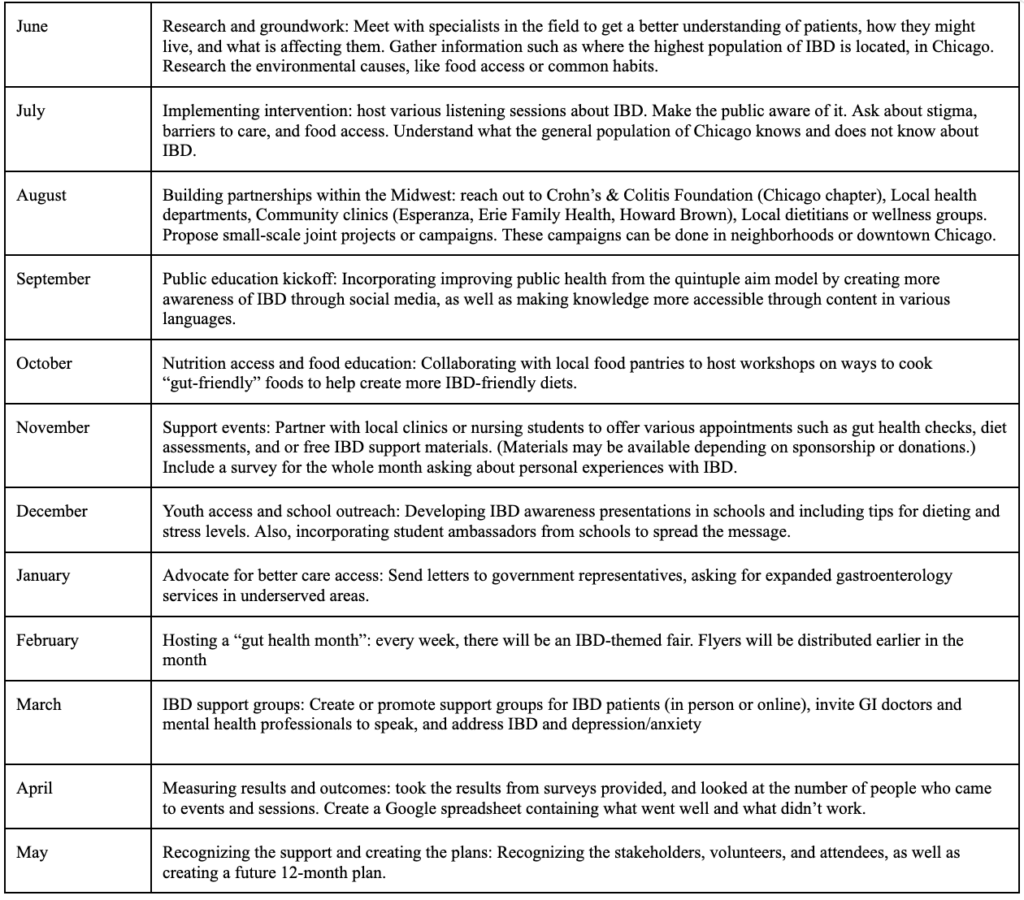
Table 3: Plan of Action
Our plan of action strives to promote IBD awareness in Chicago by hosting community-led workshops, educating students, and collaborating with local healthcare providers. We will host community workshops in Chicago neighborhoods most affected by IBD (Englewood, Austin, and West Garfield Park) to educate the population about the risk factors of IBD and how they can be prevented. By also extending these workshops to high school students, we can empower the next generation of leaders to raise awareness about IBD, which is less commonly known compared to diseases such as cancer or diabetes. Finally, collaborating with local clinics and healthcare providers will allow us to better reach underserved communities (our target population) and improve the quality of care they receive.
Strengths and Limitations
This intervention is formulated in a community-first approach. This offers a variety of lenses, from research, public engagement, future stakeholder collaboration, and culturally relevant education. One of our key strengths is our ability to incorporate multilingual content (e.g., Esperanza, Erie Family Health). Furthermore, our priorities in allowing different neighbors throughout Chicago to experience our intervention boost not only participants but also long-lasting effects. A distant strength is our integration of social determinants of health, such as food access, general stigma, and support groups. This holistic model provides tangible value by addressing not only the medical but also the social and psychological needs of IBD patients.
Despite its strengths, the intervention may face limitations such as limited funding, inconsistent community participation, and logistical challenges in collaboration across multiple sectors. Reaching underserved populations and maintaining consistent engagement, especially during later months, could be difficult without strong incentives or follow-up systems.
Discussion
In Chicago, the prevalence of IBD is increasing following national trends, which are only rising. Thousands are affected, with some of the highest prevalence and incidence rates nationwide. Health disparities caused by income inequality are widespread, with many neighborhoods having patients with limited access to gastroenterologists, delayed diagnosis of IBD, and economic constraints on healthcare expenditure. These factors all make IBD much more life-threatening in Chicago compared to other cities.
Many social determinants affect the prevalence of IBD; among them are housing, food access, and stress. These primarily influence the severity of IBD and how effective treatment is. Furthermore, there needs to be a strong support team of gastroenterologists, dietitians, and social workers to improve patient outcomes. It is important to design solutions mindful of these factors to ensure better treatment plans. Designing solutions that align with the digital health shift and the Quintuple Aim is necessary to ensure interventions are equitable. Since the Quintuple Aim prioritizes improving patient experience, advancing population health, reducing healthcare costs, supporting care team well-being, and advancing health equity, our digital symptom tracking and telehealth follow-ups enable healthcare providers to be alerted to flare-ups and improve the patient experience without significantly increasing costs. Furthermore, our social media education campaigns in multiple languages will spread awareness to wider populations and ensure that underserved demographics can achieve necessary treatment.
Our intervention plans focus on helping to support the community. This is achieved through improving research in IBD, making sure the public is engaged through various events, updating health literacy on IBD, and finally, ensuring there are support events for people with IBD. This plan will be able to sustain itself, as it will leave all participants and targets of the intervention able to remember what they learned about IBD. There will also be constant updates and revisions of the plan of action to continue to improve it and create events that will continue to help the public.
Conclusion
Inflammatory Bowel Disease (IBD) is a significant public health concern, affecting over 3 million Americans, and is continuing to grow. These numbers spike among the younger population and underserved communities. Without focused interventions, trends are expected to worsen. This may lead to deepening health disparities. Our plan of action aims to increase education on IBD and improve overall health literacy about it, enabling people to work towards preventing IBD before it occurs. We also plan to increase equity through letters to representatives to improve access to care in underserved areas, as well as creating support groups and events to help spread support for IBD. Looking at the long-term impacts, we envision this initiative expanding beyond local communities; we are working with Project Unity to spread awareness to other locations that may also have high IBD rates. For the future, studies can be conducted on finding the root causes of the rise in IBD cases for youth and marginalized populations. This can be done via research on the various factors that can lead to IBD development, such as environmental factors, diet, or stress. There can also be longitudinal studies in Chicago to see the factors that lead to the high IBD prevalence rates, along with newer initiatives, such as creating a mobile app to increase health literacy on IBD and its development. We envision our plan of action being a first step forward in helping spread awareness about this disease, along with furthering understanding surrounding all aspects of it. Hopefully, future research and awareness groups will further this mission and continue to support it.
References
- Ananthakrishnan, A. N. (2015). Epidemiology and risk factors for IBD. Nature Reviews Gastroenterology & Hepatology, 12(4), 205–217. https://doi.org/10.1038/nrgastro.2015.34
- Beaugerie, L., & Kirchgesner, J. (2019). Balancing Benefit vs Risk of Immunosuppressive Therapy for Individual Patients With Inflammatory Bowel Diseases. Clinical Gastroenterology and Hepatology: The Official Clinical Practice Journal of the American Gastroenterological Association, 17(3), 370–379. https://doi.org/10.1016/j.cgh.2018.07.013
- Borum, M. L. (2023). Racial and Ethnic Disparities in Inflammatory Bowel Disease. Gastroenterology & Hepatology, 19(5), 281–283.
- CDC. (2024, July 19). Inflammatory Bowel Disease (IBD) Basics. Inflammatory Bowel Disease (IBD). https://www.cdc.gov/inflammatory-bowel-disease/about/index.html
- CHICAGO, S. (n.d.). Sinai Chicago Inflammatory Bowel Disease Program. Sinai Chicago. Retrieved July 20, 2025, from https://www.sinaichicago.org/en/sinai-chicago-inflammatory-bowel-disease-program/
- Daneshmand, A., Du, F., & Potlach, T. (2018, May 1). Sa1750 INITIATION OF IMMUNOMODULATORS OR ADVANCED THERAPIES COMPARED TO 5ASA ALONE NOT LINKED TO INCREASED RISK OF SERIOUS INFECTIONS IN THE MEDICARE IBD POPULATOIN | Request PDF. ResearchGate. https://www.researchgate.net/publication/381222404_Sa1750_INITIATION_OF_IMMUNOMODULATORS_OR_ADVANCED_THERAPIES_COMPARED_TO_5ASA_ALONE_NOT_LINKED_TO_INCREASED_RISK_OF_SERIOUS_INFECTIONS_IN_THE_MEDICARE_IBD_POPULATOIN
- Data & Statistics. (n.d.). Illinois Department of Public Health. Retrieved July 20, 2025, from https://dph.illinois.gov/data-statistics.html
- Fehily, S. R., Al-Ani, A. H., Abdelmalak, J., Rentch, C., Zhang, E., Denholm, J. T., Johnson, D., Ng, S. C., Sharma, V., Rubin, D. T., Gibson, P. R., & Christensen, B. (2022). Review article: Latent tuberculosis in patients with inflammatory bowel diseases receiving immunosuppression-risks, screening, diagnosis and management. Alimentary Pharmacology & Therapeutics, 56(1), 6–27. https://doi.org/10.1111/apt.16952
- Gravina, A. G., Pellegrino, R., Durante, T., Palladino, G., D’Onofrio, R., Mammone, S., Arboretto, G., Auletta, S., Imperio, G., Ventura, A., Romeo, M., & Federico, A. (2023). Telemedicine in inflammatory bowel diseases: A new brick in the medicine of the future? World Journal of Methodology, 13(4), 194–209. https://doi.org/10.5662/wjm.v13.i4.194
- Hawkins, R. L., Zia, M., Hind, D., & Lobo, A. J. (2024). Inequalities in Healthcare Access, Experience and Outcomes in Adults With Inflammatory Bowel Disease: A Scoping Review. Inflammatory Bowel Diseases, 30(12), 2486–2499. https://doi.org/10.1093/ibd/izae077
- Inflammatory Bowel Disease | Chicago IBD Center—UChicago Medicine. (n.d.). Retrieved July 20, 2025, from https://www.uchicagomedicine.org/conditions-services/inflammatory-bowel-disease
- Kaplan, G. G. (2015). The global burden of IBD: From 2015 to 2025. Nature Reviews Gastroenterology & Hepatology, 12(12), 720–727. https://doi.org/10.1038/nrgastro.2015.150
- Kaplan, G. G., & Windsor, J. W. (2021). The four epidemiological stages in the global evolution of inflammatory bowel disease. Nature Reviews. Gastroenterology & Hepatology, 18(1), 56–66. https://doi.org/10.1038/s41575-020-00360-x
- Kappelman, M. D., Rifas-Shiman, S. L., Porter, C. Q., Ollendorf, D. A., Sandler, R. S., Galanko, J. A., & Finkelstein, J. A. (2008). Direct health care costs of Crohn’s disease and ulcerative colitis in US children and adults. Gastroenterology, 135(6), 1907–1913. https://doi.org/10.1053/j.gastro.2008.09.012
- Medicine, N. (n.d.). Inflammatory Bowel Disease Program. Northwestern Medicine. Retrieved July 20, 2025, from https://www.nm.org/conditions-and-care-areas/gastroenterology/digestive-health-center/inflammatory-bowel-disease-program
- Muzammil, M. A., Fariha, F., Patel, T., Sohail, R., Kumar, M., Khan, E., Khanam, B., Kumar, S., Khatri, M., Varrassi, G., & Vanga, P. (n.d.). Advancements in Inflammatory Bowel Disease: A Narrative Review of Diagnostics, Management, Epidemiology, Prevalence, Patient Outcomes, Quality of Life, and Clinical Presentation. Cureus, 15(6), e41120. https://doi.org/10.7759/cureus.41120
- Ng, S. C., Shi, H. Y., Hamidi, N., Underwood, F. E., Tang, W., Benchimol, E. I., Panaccione, R., Ghosh, S., Wu, J. C. Y., Chan, F. K. L., Sung, J. J. Y., & Kaplan, G. G. (2017). Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet (London, England), 390(10114), 2769–2778. https://doi.org/10.1016/S0140-6736(17)32448-0
- Official journal of the American College of Gastroenterology | ACG. (n.d.). Retrieved June 23, 2025, from https://journals.lww.com/ajg/abstract/2011/04000/efficacy_of_immunosuppressive_therapy_for.10.aspx
- Seligman, H. K., Laraia, B. A., & Kushel, M. B. (2010). Food Insecurity Is Associated with Chronic Disease among Low-Income NHANES Participants12. The Journal of Nutrition, 140(2), 304–310. https://doi.org/10.3945/jn.109.112573
- Singh, S., Facciorusso, A., Dulai, P. S., Jairath, V., & Sandborn, W. J. (2020). Comparative Risk of Serious Infections With Biologic and/or Immunosuppressive Therapy in Patients With Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. Clinical Gastroenterology and Hepatology: The Official Clinical Practice Journal of the American Gastroenterological Association, 18(1), 69-81.e3. https://doi.org/10.1016/j.cgh.2019.02.044
- Study Reveals Stark Racial Disparities in IBD Care Across the United States | Crohn’s & Colitis Foundation. (n.d.). Retrieved July 20, 2025, from https://www.crohnscolitisfoundation.org/study-reveals-stark-racial-disparities-ibd-care-across-the-united-states
- Zenlea, T., & Peppercorn, M. A. (2014). Immunosuppressive therapies for inflammatory bowel disease. World Journal of Gastroenterology : WJG, 20(12), 3146–3152. https://doi.org/10.3748/wjg.v20.i12.3146
Related Posts

Preventing Peripheral Artery Disease in African Americans from Georgia: A Public Health Initiative
This publication is in proud partnership with Project UNITY’s Catalyst Academy 2024...
Read More
George Washington Carver: “The Peanut Man”
Figure 1: George Washington Carver: “The Peanut Man” (Photograph ca. 1910)...
Read More
The Public Health Crisis of Alzheimer’s Disease in African American and Hispanic Populations
This publication is in proud partnership with Project UNITY’s Catalyst...
Read More
Are We Driving Our Dogs Sick Through Our Urban Lifestyles?
Figure 1: Allergic disorders in humans and dogs are associated...
Read More
Risk of Death Among Recently Released Inmates
Figure 1: While healthcare inequity is certainly an issue while...
Read More
Dancing Neurons & Their Exciting Impacts
Figure 1: A network of neurons in the brain Source: Elizabeth...
Read MoreDarius Dastur, Mishal Ali, Harshitha Ezhilarasan, Hasan Khan, Aaron Akasala