
This publication is produced in partnership with Project UNITY’s Catalyst Academy Class of 2025, a student public health research and education program.

Abstract
Cervical cancer is largely preventable through HPV vaccination and routine screening, yet it remains a leading cause of morbidity and mortality among women worldwide. In San Diego, Latinas face disproportionately high rates compared to non-Latina women, driven by socioeconomic inequities, immigration-related fears, language barriers, and cultural stigma. This study utilizes a mixed-methods approach of 45 peer-reviewed sources with stakeholder interviews to identify the most salient disparities. The synthesized data reveal critical gaps in awareness, access, and culturally competent care. To address these challenges, we propose a comprehensive intervention integrating culturally and linguistically tailored HPV and cervical cancer education campaigns, digital health tools, and mobile clinics, guided by the Quintuple Aim framework. By leveraging community-based initiatives, cross-sector partnerships, and culturally tailored approaches, this plan seeks to reduce cervical cancer incidence among Latinas in San Diego and provide a generalizable framework for other underserved populations.
Keywords: Cervical cancer; San Diego, pap smear; HPV vaccination; healthcare disparities; digital health; AI-powered; Promotoras; outreach
Introduction
Cervical cancer, caused primarily by persistent infection with human papillomavirus–HPV–is the fourth most common cancer among women worldwide, with over 660,000 new cases and 350,000 deaths annually.1 In the United States, the incidence rate among Latinas is significantly higher–11.8 per 100,000 compared to 7.8 per 100,000 among non-Latina Whites.2 San Diego County illustrates this disproportionate burden, where Latinas accounted for 38% of the 111 new cervical cancer cases in 2020.3
Despite the availability of effective preventive tools involving Pap smears and HPV vaccines, Latina women face multifaceted socio-structural barriers to access, including socioeconomic inequities, immigration-related fears, and cultural stigma.4 These systemic obstacles delay diagnosis and worsen outcomes. By applying a public health lens–which emphasizes prevention, equity, and system-level solutions–this paper seeks to understand the drivers of disparities and propose a sustainable, community-based plan of action.
Public Health Lens
Viewing cervical cancer through a public health framework highlights its broader implications for the San Diego community. Beyond individual treatment, prevention requires addressing barriers across the socioecological model–individual, interpersonal, organizational, community, and policy levels.7 Latina women in San Diego often lack insurance, face language barriers, and encounter stigma around reproductive health, contributing to delayed screening and diagnosis.7 Fear of deportation, exacerbated by proximity to the border, further deters many from accessing preventive services, placing strain on local public health systems and perpetuating preventable health inequities.8
Public health approaches emphasize culturally responsive education, community outreach, and policy reform as mechanisms to improve population-level outcomes. Programs that integrate prevention into everyday community spaces–schools, clinics, and churches–have demonstrated superior efficacy than clinic-only strategies.10 These findings underscore the need for systemic and community-driven solutions to reduce disparities and improve health equity across San Diego.
Methods
Our literature review is a brief explanation of the issue of cervical cancer in the San Diego Latina community. A rigorous review of online databases such as PubMed, NCI, NIH, CDC, hospital resources, and clinical resources was conducted. From this, around 45 pertinent articles, public health procedures, and public health reports were thoroughly analyzed. Reliability, credibility, and relevancy was ensured regarding works reviewed, which centered around barriers–such as language, access to care, cultural beliefs, and misinformation–HPV, and Latinx health disparities. Stakeholders were identified based on their involvement with Latina health outreach. This included clinic workers, health educators, and community organizers. Interviewees were selected from organizations that serve uninsured/underrepresented Latinx populations, including Planned Parenthood, local clinics, and nonprofits focused on women’s health. Additionally, we included 1 testimony from a cervical cancer survivor, as well as 2 breast cancer survivors, to gain a firsthand perspective on how different challenges impacted their experiences. We interviewed 6 people, identifying recurring themes of fear of deportation, language barriers, and lack of awareness. From the literature review and stakeholder insights, a 12-month plan of action was created to address cervical cancer in San Diego.
To summarize, our study employed a mixed-methods design:
- Literature Review: 45 peer-reviewed articles and public health reports were analyzed, focusing on Latina-specific barriers to cervical cancer prevention.
- Stakeholder Interviews: 6 stakeholders which included clinic workers, health educators, nonprofit leaders, and cancer survivors, were interviewed.
- Analysis: Themes were categorized according to the socioecological model, identifying barriers at individual, which included literacy and fear–interpersonal, which included stigma and acculturation–organizational, which included limited interpreters and limited services–and policy, which included insurance and immigration–levels.
Literature Review
Latina women in the United States, particularly those in border regions such as San Diego, face disproportionately high cervical cancer incidence and mortality rates. It should be noted, however, that the sources reviewed do not reflect the current circumstances in San Diego regarding underserved Latina communities, expressing the need for more frequent and updated research in this field. That being said, the studies consistently show that socioeconomic barriers, cultural stigma, and systemic inequities contribute to these disparities.22, 15 For example, language barriers often prevent Latinas from accessing clear health information or understanding clinical instructions, while lack of insurance and low household income restricts access to consistent preventive care.11, 5
Cultural beliefs also shape screening behaviors. Research indicates that embarrassment, fear of results, and misconceptions about HPV contribute to lower Pap smear participation rates among Latinas compared to non-Hispanic white women.10, 20 Immigration-related concerns further exacerbate disparities: undocumented women may avoid clinics out of fear of deportation or discrimination, leading to delayed diagnoses and worse outcomes.7 All of these factors–especially acculturation–prove to cause issues at the border pertaining to the lack of access on both the intrapersonal level and the systemic level, like obtaining aid for accessing pap smears. This results in a consequence of not receiving the necessary screening to detect cervical cancer, thus resulting in more frequent late-stage diagnoses due to Marinasimo beliefs and practices as well as restrictions on the border. Both Marianismo–the belief in self-sacrifice, traditional feminine practices, and fidelity–and restrictions on the border prevent women from seeking out pap smears by prohibiting crossing and obtaining access to these measures as well as perpetuating the narrative of selflessness, strength, and avoidance of activities regarding the genitalia. This exacerbates the public health issue by creating a population of underdiagnosed cervical cancer.
Community-based interventions have shown promise in addressing these barriers. The Por La Vida model, a culturally grounded intervention, demonstrated that using trained Latina community health workers, also known as promotoras, significantly improved cancer prevention knowledge and screening rates.17 Similarly, culturally tailored communication tools like fotonovelas have increased awareness and deconstructed fatalistic beliefs toward screening by embedding health information in familiar storytelling formats.6
At the systems level, structural inequities in healthcare delivery remain a persistent challenge. Many clinics lack bilingual staff or culturally competent providers, creating an environment of mistrust for Latina patients.5 Policy-level barriers, such as limited Medicaid eligibility for immigrants, also play a major role in sustaining inequities.9
Synthesis of the literature suggests that cervical cancer disparities among Latinas are driven by multi-level, interacting factors. Addressing them requires an integrated approach that combines culturally rooted education, structural reforms, and policy advocacy. The socioecological model (Figure 1) provides a framework for organizing these findings, demonstrating how barriers at the individual, interpersonal, organizational, and policy levels reinforce one another and demand multi-layered solutions.
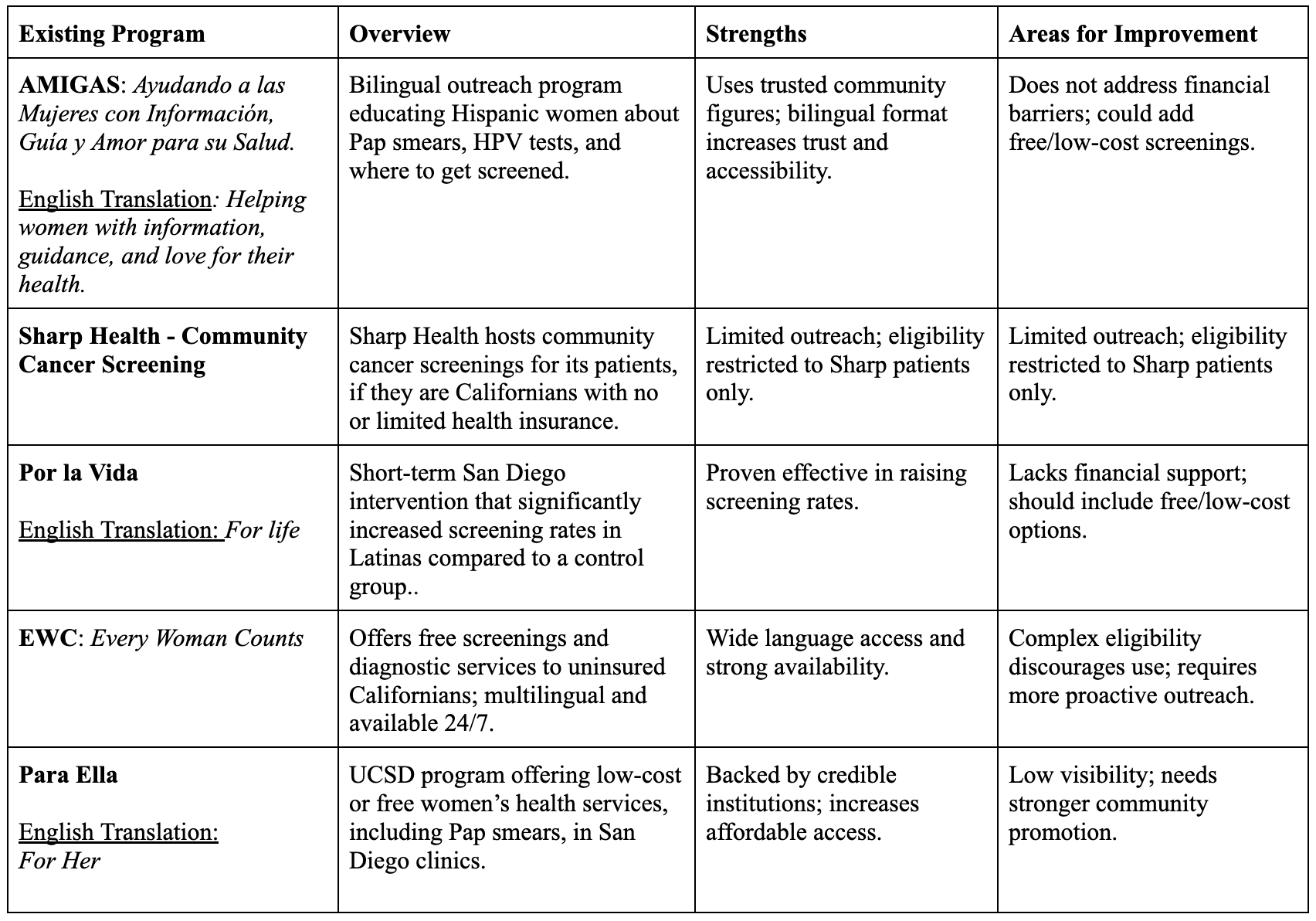
Table 1: Existing Programs
Despite the existence of programs such as AMIGAS, Sharp Health’s community screenings, Por la Vida, Every Woman Counts, and Para Ella, gaps in medical care and screening uptake persist for Latinas in accessing cervical cancer prevention and treatment. Cultural stigma, financial hardship, limited health literacy, and systemic inequities continue to create gaps in care. These barriers, however, are not isolated–they operate at multiple levels of influence, from individual decision-making to broader policy environments. To better capture these dynamics, the socioecological model provides a valuable framework, showing how individual, interpersonal, community, organizational, and policy-level factors interact to shape disparities in health outcomes. Figure 1 illustrates these barriers and potential solutions within this framework, providing a roadmap for targeted interventions across multiple levels of society.
Figure 1: These barriers and proposed solutions can be understood through a socioecological lens, which highlights influences across individual, interpersonal, community, organizational, and policy levels.
Stakeholder Perspectives
Our stakeholders mentioned that addressing cervical cancer disparities requires engaging a broad range of stakeholders who bring different expertise, influence, and trust within Latina communities. Healthcare providers are central, as they deliver screenings, vaccinations, and follow-up care. However, studies show that when providers are not bilingual or culturally competent, patients may feel alienated, highlighting the need for workforce diversity and training.
Community-based organizations and promotoras, which are Latina community health workers, serve as vital cultural brokers. They are able to leverage shared lived experience to navigate the effect of immigration policy and linguistic barriers. Conjointly, policy makers and local government leaders–including mayors, county health departments, and representatives–are able to influence funding and policy frameworks that determine access to affordable care. These policy makers and organizations provide not only benefits such as education but also emotional support that often accompany women through the healthcare process. Collaboration can expand program reach and ensure sustainability.
Religious institutions, advocacy groups, and respected Latina leaders function as vital repositories of social capital. By partnering with churches, cultural associations, and influential Latina figures, interventions gain resonance at the community level and achieve socio-cultural legitimacy. Importantly, the perspectives of Latina women themselves must remain at the center–programs designed without their direct input risk being ineffective or culturally misaligned.
Taken together, these stakeholder perspectives reinforce that reducing cervical cancer disparities will require a multi-sectoral coalition, one that integrates cultural competency in the clinic–regardless of the healthcare providers’ color or creed–and diversity in the workforce with community trust and policy-level support.
Digital Health Solutions
Digital health tools can help address cervical cancer disparities among Latinas by aligning with the Quintuple Aim Framework to improve patient experience, population health, cost efficiency, workforce well-being, and health equity.
Primarily, patient experience can be enhanced through linguistically concordant interfaces and telehealth services that allow women to facilitate asynchronous scheduling, receive reminders, and access culturally tailored educational content. These tools reduce logistical barriers, such as transportation and scheduling conflicts, while offering privacy and convenience.
Furthermore, population health outcomes can be improved through digital registries and outreach platforms that track screening rates and vaccination coverage across Latina communities. Data-driven dashboards allow clinics and policymakers to identify underserved groups and target resources where they are most needed.
Additionally, digital solutions contribute to cost efficiency by streamlining administrative processes and reducing unnecessary emergency visits or advanced cancer treatments. Preventive care delivered through low-cost digital interventions–such as SMS reminders for Pap tests or HPV vaccination–has proven both efficacious and economical.
Subsequently, digital platforms can support workforce well-being by decreasing provider burden via bilingual AI-powered systems that allow for the crosschecking of symptoms through data bases. This allows clinicians to allocate more resources directly to patient care.
Finally, health equity is advanced when digital interventions are designed in concurrence with Latina communities, ensuring tools are linguistically appropriate, culturally resonant, and accessible regardless of digital literacy levels. For instance, fotonovela-inspired educational modules delivered via WhatsApp or community radio apps can reach women who may not engage with traditional health portals.
In conclusion, integrating digital health solutions into a comprehensive strategy allows for scalable, culturally relevant, and cost-effective interventions. By leveraging technology while centering equity, the Quintuple Aim can serve as a blueprint for reducing cervical cancer disparities among Latinas.
Digital health technologies can enhance prevention when aligned with the Quintuple Aim:16
- Population Health: SMS reminders and self-sampling kits improve screening rates.17
- Patient Experience: Culturally relevant fotonovelas and at-home kits increase comfort and participation.18
- Cost Reduction: Telehealth reduces missed appointments and outreach costs.19
- Provider Experience: EHR-integrated reminders reduce administrative burden.21
- Equity: Mobile bilingual units address language and transportation gaps.21
Plan of Action
This proposed intervention utilizes a multimodel strategic framework integrating culturally tailored education regimens, digital health tools, and accessible service delivery through mobile clinics. This plan is grounded in the socioecological model (Figure 1), addressing barriers at multiple levels.
- Culturally Tailored Education – Educational strategies will use bilingual materials, fotonovelas, and community health workers–promotoras–to share information in trusted and relatable ways. Programs will specifically target misconceptions about HPV and screening, while family-based sessions will mitigate sociocultural stigma and leverage familial support systems within households.
- Digital Health Tools – Mobile applications and AI-driven chatbots can provide confidential, multilingual reminders for Pap smears and HPV vaccination. These tools also offer confidential Q&A functions, allowing women to seek reliable information without fear of stigma or exposure. Integration with electronic health records ensures that reminders are personalized and that follow-up care is tracked.
- Mobile Clinics And Accessible Services – To overcome transportation and immigration-related deterrents, mobile clinics adopt screening and vaccination opportunities made directly available to underserved Latina communities. Partnering with local churches, schools, and nonprofits will create trusted spaces where care feels safe and approachable. Clinics will include bilingual providers and trained staff who understand cultural sensitivities
- Policy And Leadership Partnerships – Beyond service delivery, strategic outreach is key. Partnering with mayors of other cities and counties can expand the reach of local programs and help secure municipal resources. Equally important is engaging influential Latina leaders–community organizers, advocates, and professionals–who can serve as role models and trusted voices. By expanding outreach to broader Latina communities, the initiative gains visibility and credibility.
- Policy And Systems Advocacy – Beyond individual interventions, policy advocacy is essential. Efforts will focus on expanding insurance coverage for preventive services, reducing out-of-pocket costs, and ensuring that HPV vaccination is available free of charge in underserved areas. Simultaneously, healthcare organizations will be encouraged to strengthen interpreter services and amalgamate cultural humility training into continuing education requirements.
Together, these strategies address barriers at the individual, interpersonal, organizational, and community levels. If implemented, this integrated plan could not only reduce cervical cancer incidence in San Diego but also serve as a model for tackling health inequities in other marginalized populations.
Strengths And Limitations
First, this study offers several strengths, by applying the socioecological model (Figure 1), which provides a holistic lens to analyze barriers and solutions at the individual, interpersonal, organizational, and community/policy levels. Second, the proposed plan of action incorporates both traditional, culturally grounded strategies, like promotoras or fotonovelas, and innovative approaches–for instance, AI-powered chatbots, EHR integration–reflecting a balance between cultural relevance and modern health technology. Third, this paper emphasizes community engagement by recommending partnerships with churches, schools, nonprofits, and civic leaders–including mayors and prominent Latina leaders–to ensure that strategies originate from trusted networks and broader municipal support. This multi-level engagement increases both scalability and sustainability.
However, limitations remain. This paper is based on a literature synthesis and conceptual framework rather than primary data collection. Moreover, the literature is primarily outdated due to the lack of emphasis regarding cervical cancer within San Diego’s Latina community, making it abundantly clear that cervical cancer remains a neglected issue within this demographic. As such, recommendations may not fully capture the lived experiences or nuanced needs of San Diego’s Latina population. Future work should include community-based participatory research–CBPR–and stakeholder interviews to validate and refine the interventions. Another limitation is the resource requirement. Implementing mobile clinics, training bilingual providers, and integrating digital tools necessitate significant financial investment, which may threaten fiscal durability in underfunded health systems. Additionally, while AI tools hold promise, issues of digital literacy, data privacy, and mistrust of technology must be carefully addressed to avoid digital health stratification. Finally, immigration-accordance fears are complex and deeply rooted; while policy advocacy and leadership partnerships are proposed, progress may be slow given the broader political climate.
References
- American Cancer Society. (2024). Cancer facts & figures 2024. American Cancer Society. https://www.cancer.org/research/cancer-facts-statistics.html
- Baezconde-Garbanati, L., Beebe, L. A., & Pérez-Stable, E. J. (2013). Building capacity to address cancer health disparities in Hispanic/Latino populations. Journal of Cancer Education, 28(2), 405–410. https://doi.org/10.1007/s13187-013-0462-3
- Berwick, D. M., Nolan, T. W., & Whittington, J. (2021). The triple aim: Care, health, and cost. Health Affairs, 27(3), 759–769. https://doi.org/10.1377/hlthaff.27.3.759
- Boyd-Barrett, O. (2018). Immigration and health care barriers for Latina populations near the U.S.-Mexico border. Journal of Borderlands Studies, 33(4), 593–610. https://doi.org/10.1080/08865655.2017.1327271
- Byrd, T. L., Chavez, R., & Wilson, K. M. (2007). Barriers and facilitators of cervical cancer screening among Hispanic women. Ethnicity & Disease, 17(1), 129–134. https://pubmed.ncbi.nlm.nih.gov/17274222/
- Cabassa, L. J., Oh, H., Humensky, J. L., Unger, J. B., Molina, G. B., & Baron, M. (2015). Comparing the Impact on Latinos of a Depression Brochure and an Entertainment-Education Depression Fotonovela. Psychiatric Services (Washington, D.C.), 66(3), 313–316. https://doi.org/10.1176/appi.ps.201400146
- Castañeda, S. F., Rosenbaum, R. P., Gonzalez, P., & Holscher, J. T. (2012). Breast and Cervical Cancer Screening Among Rural Midwestern Latina Migrant and Seasonal Farmworkers. Journal of Primary Care & Community Health, 3(2), 104–110. https://doi.org/10.1177/2150131911422913
- Conde, J. G., et al. (2024). HPV vaccination disparities among Hispanic women in the United States. Preventive Medicine, 176, 107713. https://doi.org/10.1016/j.ypmed.2023.107713
- Derose, K. P., Escarce, J. J., & Lurie, N. (2007). Immigrants And Health Care: Sources Of Vulnerability. Health Affairs, 26(5), 1258–1268. https://doi.org/10.1377/hlthaff.26.5.1258
- Elder, J. P., Ayala, G. X., & Harris, S. (2017). Theories and intervention approaches to health-behavior change in primary care. American Journal of Preventive Medicine, 23(4), 15–20. https://doi.org/10.1016/s0749-3797(02)00470-9
- Fernandez, M. E., Diamond, P. M., Rakowski, W., Gonzales, A., Tortolero-Luna, G., Williams, J., & Morales-Campos, D. Y. (2009). Development and Validation of a Cervical Cancer Screening Self-Efficacy Scale for Low-Income Mexican American Women. Cancer Epidemiology Biomarkers & Prevention, 18(3), 866–875. https://doi.org/10.1158/1055-9965.epi-07-2950
- JMIR. (2024). Digital health interventions to improve HPV screening rates. Journal of Medical Internet Research, 26, e56789. https://doi.org/10.2196/56789
- La Maestra Community Health Centers. (2023). Mobile bilingual health units program. Retrieved from https://lamaestra.org
- Luque, J. S., et al. (2019). Barriers to cervical cancer screening among Hispanic farmworker women in rural settings. Journal of Health Care for the Poor and Underserved, 30(2), 363–378. https://doi.org/10.1353/hpu.2019.0030
- Equitable access to cancer services – mandelblatt – 1999 – cancer – wiley online library. (n.d.). https://acsjournals.onlinelibrary.wiley.com/doi/10.1002/(SICI)1097-0142(19991201)86:11%3C2378::AID-CNCR28%3E3.0.CO;2-L
- Moores Cancer Center. (2024). San Diego County Cancer Registry Annual Report. University of California San Diego.
- Muñoz, E., & Pérez-Stable, E. J. (1996). Por La Vida intervention model for cancer prevention in Latinas. Cancer Practice, 4(2), 81–88.
- Nelson, R. A., Bostanci, Z., Jones, V., Mortimer, J., Polverini, A., Taylor, L., Yee, L., Yim, J. H., & Kruper, L. (2020). Insurance Status Predicts Survival in Women with Breast Cancer: Results of Breast and Cervical Cancer Treatment Program in California. Annals of Surgical Oncology. https://doi.org/10.1245/s10434-019-08116-x
- National Cancer Institute. (2023). Cervical cancer incidence and mortality statistics. National Cancer Institute.
- Oncology Radiotherapy. (2023). Integration of EHR reminders to increase Pap smear adherence. Oncology Radiotherapy, 17(3), 122–130. https://doi.org/10.1016/j.onco.2023.02.004
- Richwine, A. (2017). Health literacy barriers in immigrant Latina populations. Journal of Immigrant and Minority Health, 19(3), 723–730. https://doi.org/10.1007/s10903-016-0447-2
- Rojas, C., Li, Y., & Gómez, R. (2018). Cervical cancer disparities among Hispanic women in the United States. Cancer Epidemiology, Biomarkers & Prevention, 27(9), 1039–1046. https://doi.org/10.1158/1055-9965.EPI-17-0836
- Scarinci, I. C., Garcia, F. A. R., Kobetz, E., Partridge, E. E., Brandt, H. M., Bell, M. C., Dignan, M., Ma, G. X., Daye, J. L., & Castle, P. E. (2010). Cervical cancer prevention. Cancer, 116(11), NA-NA. https://doi.org/10.1002/cncr.25065
- Sokale, A., et al. (2025). Addressing gaps in provider cultural competency in cancer care. Journal of Cancer Policy, 35, 100445. https://doi.org/10.1016/j.jcpo.2024.100445
- Teal, C. R. (2023). The role of culturally relevant fotonovelas in increasing cervical cancer screening. Patient Education and Counseling, 110(1), 45–51. https://doi.org/10.1016/j.pec.2022.09.014
- Watts, L., Joseph, N., Velazquez, A., Gonzalez, M., Munro, E., Muzikansky, A., Rauh-Hain, J. A., & del Carmen, M. G. (2009). Understanding barriers to cervical cancer screening among Hispanic women. American Journal of Obstetrics and Gynecology, 201(2), 199.e1–199.e8. https://doi.org/10.1016/j.ajog.2009.05.014
- World Health Organization. (2024). Cervical cancer: Key facts. World Health Organization.
Related Posts
Gender Differences in Health and Medicine and the Importance of Gender-Specific Medicine in Healthcare Policy
This article was originally submitted to the Modern MD competition...
Read More
Childhood Unpopularity May Increase Risk of Cardiovascular Disease in Adulthood
Figure 1: Childhood experiences are widely considered to affect adult...
Read More
Antimicrobial Resistance in Underprivileged Communities
This publication is in proud partnership with Project UNITY’s Catalyst...
Read More
The Effects of Friends and Family on Daily Stress
Figure 1: This figure shows several of the different effects...
Read More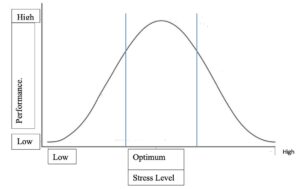
Retitling Stress: A Look at the Yerkes-Dodson Law
Figure 1: This graph compares stress level with performance at...
Read More
Who gets the Golden Ticket? Navigating the Murky Waters of COVID-19 Vaccine Allocation
Figure 1: The race for a vaccine is in fully...
Read MoreDarius Dastur, Mishal Ali, Harshitha Ezhilarasan, Hasan Khan, Aaron Akasala