
This publication is produced in partnership with Project UNITY’s Catalyst Academy Class of 2025, a student public health research and education program.

Abstract
Generalized anxiety disorder (GAD) is among the most common mental health conditions affecting adolescents aged 13–18 in the United States. San Diego, California, exhibits particularly high rates of GAD among low-income, Latino, LGBTQ+, and female students. Although school-based services and community programs are available, teens often face major barriers, such as stigma, cultural differences, and a lack of awareness. If left untreated, GAD may severely affect academic performance, social skills, and long-term mental health. This report investigates the national and local rates of GAD among adolescents and suggests a community-based intervention to improve access to care. This research comes from a review of articles, government reports, and community data from databases including PubMed and Google Scholar. Interviews with mental health professionals in San Diego were conducted to provide real-world insights to the findings, which report that GAD has a greater impact on teens from marginalized groups due to limited access to culturally appropriate care, stigma, financial challenges, and school counselor shortages. Current interventions often overlook these groups due to poor organization and low participation. The proposed solution is a digital platform with peer-led “Digital Navigators” trained in Youth Mental Health First Aid. A list of resources for GAD will consist of a resourceful chatbot; contact information of GAD specialists in San Diego based on preferred language, race, gender, or ethnicity; and credible medical information on GAD. Ultimately, this multi-pronged strategy aims to improve access, reduce stigma, and encourage teens to support one another, with the goal of reshaping how youth in San Diego connect with mental health services.
Keywords: GAD; adolescents; high schoolers; San Diego; digital mental health; peer-based intervention; mental health; public health
Introduction
Generalized anxiety disorder (GAD) is among the most prevalent mental health conditions among adolescents, affecting approximately 5% of U.S. youth aged 13-18, according to Boston Children’s Hospital.1 GAD is characterized by a persistent, excessive worry that interferes with daily functioning. It is often accompanied by physical symptoms such as fatigue, irritability, and difficulty concentrating. When left untreated, GAD increases the risk of depression, substance use, and suicidal ideation, making early interventions critical. GAD is particularly prevalent in urban areas such as San Diego, where one in eight youth experienced some form of GAD or depressive episode. Despite its prevalence, only 20% of adolescents report receiving mental health therapy, and 16% report taking a prescription for their mental health.2
Key factors that contribute to GAD disparities include cultural stigma, financial barriers, and structural challenges in already established mental health resources. Marginalized groups, such as LGBTQ+ and low-income youth, face disproportionately high rates of undiagnosed GAD due to system inequities.6 Economically, untreated adolescent anxiety costs the U.S. hundreds of billions of dollars annually in healthcare expenses and lost productivity.3 These costs could exponentially increase in San Diego, where mental health resources are found across clinics, schools, and non-profits, causing many families to struggle in navigating personalized care.
To address this crisis, improving mental health literacy, resource accessibility, and early intervention is critical. This report examines the distribution of GAD in San Diego youth, analyzes systemic barriers to care, and proposes a digital navigator platform to centralize mental health resources that can be tailored to an individual’s culture, orientation, and personality traits. By combining national data with local disparities, this report aims to highlight solutions that can reduce the long-term individual and societal impacts of untreated anxiety.
Public Health Lens
In San Diego, teenagers struggling with GAD often face barriers to care not because of a lack of resources, but due to limited awareness and accessibility to existing resources. Nationally, approximately 32% of teens in the U.S. struggle with anxiety, yet only a small percentage receive treatment.4 Locally, about 14.6% of clients in San Diego with mental health treatments are diagnosed with anxiety; however, the disorder remains underdiagnosed, especially among ethnic minorities.5 Diagnosis is further delayed by structural barriers such as uneven distribution of providers, insurance limitations, cultural stigma around mental health, and lack of accurate knowledge.6
As a result, addressing this issue through a public health lens is crucial to combat these disparities. Social determinants such as low income, housing instability, and lack of health insurance correlate with a higher risk of GAD and a decreased likelihood of utilizing resources.7 Viewing GAD through this framework pushes public health efforts to focus on primary prevention, reducing cultural stigma, integrating mental health into communities, and expanding equitable access. These strategies are proven to improve long-term outcomes beyond the medical model alone.
Methodology
A systematic literature review of 28 peer-reviewed government reports, local sources in San Diego, and other scholarly sources explored the prevalence, impacts, and service gaps of GAD among U.S. adolescents, with a focus on San Diego County. Searches prioritized keywords such as “adolescent GAD prevalence in the U.S.,” “academic impairment through mental health disorders,” and “mental health service utilization barriers in San Diego.” The sources were primarily analyzed on: (1) U.S.-based epidemiological data in San Diego, (2) measurable academic and mental health outcomes, and (3) evaluation of intervention efficacy. Studies that focused on non-U.S. populations, lacked adolescent-specific data, or were based on small samples were excluded. The review was split into a national literature review and a justification of the target population. The national literature review compiled national data2 allowing for a contextualization of broader trends. Similarly, the justification of the target population focused on local sources,5,7,8 which revealed regional trends in teen utilization and access to mental health resources.
Additionally, two stakeholders were interviewed to gain real-world insight into how GAD affects teenagers in San Diego and how various organizations in San Diego respond to these mental health crises. first began researching different mental health facilities, psychologists’ offices, and school-based mental health programs in San Diego. Through research, identified and contacted approximately13 professionals who could offer their expertise on GAD in teenagers (ages 14-18). After compiling data from the two interviews, a qualitative analysis was conducted by identifying patterns in the responses of the stakeholders, including common barriers like stigma, lack of awareness around available resources, and demographic inequalities.
Literature Review
Generalized anxiety disorder (GAD) is a growing public health concern in the United States, affecting around 10-20% of adolescents aged 15 to 20.9 The COVID-19 pandemic exacerbated this issue, with a 25% increase in the prevalence of mental disorders, especially GAD. Female adolescents experience GAD at approximately twice the rate of males. Similarly, youth from low-income households face disproportionate barriers to treatment access.9,10 GAD also contributes to the frequency of mental health comorbidities, such as Major Depressive Disorder (MDD) and migraines. In the educational sphere, students with GAD demonstrate 15 to 22% higher rates of test anxiety and a greater likelihood of course failure.11 Older adolescents, such as college students, also show elevated levels of suicidal ideation connected with untreated anxiety.12
Despite the increased availability of resources and interventions from educational institutions, the actual utilization of these services hinders their desired efficacy. Data from safety-net hospitals indicate that fewer than 50% of publicly insured youth fail to attend their first psychiatric appointments. Additionally, controlled studies of Michigan school programs found no significant difference in the students’ mental health and well-being across various implementation methods, highlighting the failures in engagement strategies in current mental health resources, rather than resource scarcity.10,13 However, there are promising exceptions, such as the Health Minds, Thriving Kids program, which employs a skill-building approach that has enabled more than 80% of its respondents to acquire useful strategies for emotional management, coping, and addressing negative thinking patterns.8 These findings underscore the need for targeted reforms to address the clinical quality and structural inequities in adolescent mental healthcare and well-being services.
Our research team consists of members from Danville, California, and San Diego, California, and identified San Diego as having the highest rates of GAD among the areas studied. The county has experienced a significant increase in the number of behavioral and mental health issues among youth, including symptoms of GAD. There is growing clinical recognition of conditions related to the diagnosis of stress-associated anxiety, which increased from 9% in fiscal year (FY) 2018–19 to 15% in FY 2022–23.7 Rady’s Children’s Hospital reported that in 2021, teen mental health visits increased by 25%, further displaying the severity of these conditions.14 Data collected from the San Diego Unified School District also shows that 35.1% of students aged 14 to 18 reported feeling persistent sadness or hopelessness for two or more weeks at a time.15 These emotional stress indicators are connected to GAD symptoms such as chronic worry and fatigue. All of these local statistics from this region alarmingly prove how much of a common and growing problem GAD is becoming among adolescents in San Diego, and how there must be more calls for action to address this crisis.
Furthermore, GAD rates are disproportionate in some San Diego County areas and demographic groups more than others. East San Diego recorded the highest inpatient discharge rate for teen mental health issues at 874 per 100,000 adolescents, while North Coastal recorded the highest ER rate for women between the ages of 15 and 24 at 514 per 100,000 individuals. Additionally, female high school students in the San Diego Unified School District report more than twice the rate of emotional distress (44.2%) as male students (22.1%). Furthermore, Latino high school students reported the highest amount of emotional distress at 39.6%15, and 43% of LGBTQ+ adolescents reported anxiety symptoms. This gender inequity is reflected on a global scale as well.16
A teen’s risk of developing or managing GAD in San Diego is significantly influenced by personal factors such as stress management, sleep patterns, and poor financial situations. The 2024 San Diego County Ideas Lab Report found that 74.5% of teenagers linked their mental distress to sleep deprivation, and 82.3% concluded that academics mainly influenced their anxiety.17 This data is backed by studies that relate fewer hours of sleep to less productivity and heightened anxiety. Additionally, 25% of San Diego’s population suffers from inadequate nutrition due to unstable financial circumstances, with over 212,000 people being children, making it difficult for low-income families to maintain mental health,18 leading to GAD.
Interpersonal factors, including family dynamics, peer relationships, and social systems, are crucial to understanding how youth manage GAD. Research shows that a certain home environment, such as growing up with a parent who is over-controlling, rejecting, or anxious themselves, is correlated to the risk of youth developing anxiety. For example, children of anxious parents are nearly twice as likely to develop anxiety, with the over-controlling parent being a key contributor.19 Furthermore, adolescents who receive limited affection or high criticism from their parents often experience more difficulty managing their anxiety.20 Social support is also crucial – this plays a role in the long term, as adolescents with strong social support report fewer anxiety symptoms during adulthood.6 However, adolescents with social anxiety face significant barriers to accessing treatment, particularly when social support is limited. Prior research indicates that only a small minority of socially anxious adolescents seek professional help for their symptoms.21
Schools and local organizations in San Diego are pivotal in how adolescents view and treat mental health issues, including GAD. While these organizations have ample resources, they often face accessibility challenges that limit their ability to provide sufficient help. For example, California’s student-to-counselor ratio averaged 376:1 during the 2023–2024 school year, way above the American School Counselor Association’s (ASCA) recommended ratio of 250:1.22In response to an increase in demand for mental health services post-COVID-19, California’s Children and Youth Behavioral Health Initiative funded a wellness coach program. In San Diego specifically, the San Diego Unified School District received $950,000 to fund 10 wellness coaches across schools, to ease the burden on school counselors and social workers. However, since these coaches are nonclinical staff and tend to rotate between multiple schools, they are often unable to offer thorough, individualized support. Additionally, following the pandemic, a 2021 survey conducted by ACLU found that only 17% of students reported an increase in mental health services at their schools, while an alarming 83% saw no improvement in access. Barriers such as peer and parent stigma, limited staff, and lack of connection with providers were key reasons students did not seek help.23
San Diego community-level determinants significantly influence the etiology and management of GAD for adolescents. The San Diego Youth Services provides subsidized clinical interventions, including therapy and housing support, serving a cohort of over 28,000 young people every year.5 Despite this, there are substantial adolescent populations in underserved communities such as East County and South Bay who encounter systemic impediments to receiving care, such as limitations in transportation, language differences, and stigma surrounding mental health. Proximity to green spaces and community programs can also help teens manage anxiety. Programs such as Park Rx San Diego promote emotional wellness by encouraging time spent in nature, which has been shown to reduce stress. Yet, some areas, such as Logan Heights and City Heights, have fewer parks, making it harder for teens in those neighborhoods to benefit from these resources.24 Belonging to and connecting with the community is also a protective factor against teens developing severe anxiety, specifically faith-based groups, cultural organizations, and after-school programs. Local reports show persistent gaps in youth engagement with community-based mental health services in San Diego County, highlighting ongoing gaps in service uptake.8 While many resources exist, they are not always accessible or culturally inclusive enough to reach the teens who need them most.
Policies at the local, state, and national levels all affect how GAD is treated and prevented in San Diego teens. At the federal level, programs like the Mental Health Services Block Grant and laws expanding mental health coverage have helped facilitate access to care. But for many teens from undocumented or mixed-status families, insurance limitations and fear of seeking help impede access to care. Alarmingly, fewer than half of students who were referred to mental health services through schools follow through with treatment.25 Statewide, California has made efforts to address this through initiatives like the Behavioral Health Continuum Infrastructure Program, which invests in school-based mental health support. Despite launching broader efforts, such as the Live Well San Diego Initiative, San Diego Unified is facing critical workforce deficits of mental health professionals and resource accessibility due to oversight, limited access to culturally competent providers, and language barriers.26
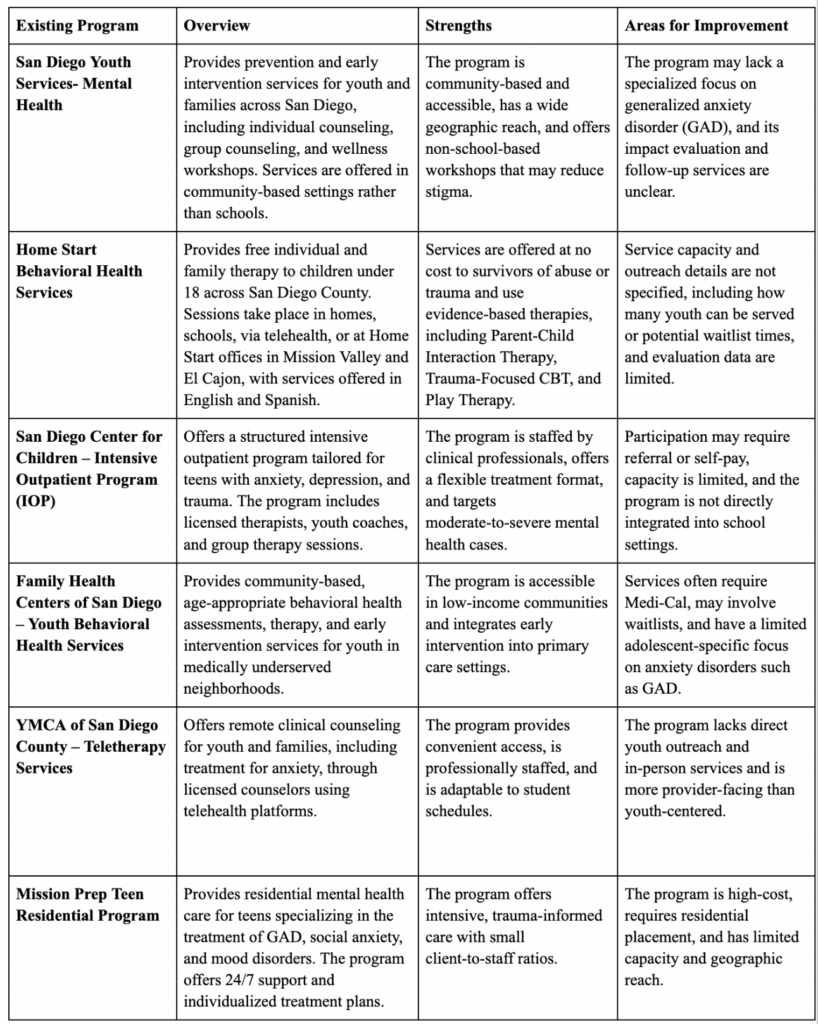
Table 1: Overview of GAD Programs for Adolescents (14–18) in San Diego
Stakeholder Perspectives
For stakeholder insights, two key experts were interviewed. Dr. Dani Schaer, a psychologist specializing in teenage mental health, noted that while GAD diagnoses are increasing, overdiagnosis may sometimes blur the line between normal stress and clinical anxiety. She emphasized that stigma and discomfort often prevent teens from seeking help and recommended integrating school support tools to make resources more accessible. Ms. Alex Swanson, program manager at Sunny Days at San Diego Youth Services, highlighted the barriers faced by teens in low-income areas, including stigma, distrust of systems, and limited access to phones, the internet, or transportation. She suggested that our intervention also incorporate tools that offer nutrition and physical activity recommendations, and grounding techniques to better meet teen needs and increase engagement. Together, their perspectives helped us shape a more practical and inclusive intervention model.
Digital Health Solutions
The Quintuple Aim model provides a comprehensive framework for addressing healthcare challenges by focusing on improving population health, enhancing patient experience, reducing costs, improving healthcare provider experiences, and advancing health equity. This model is a framework that guides digital solutions addressing systemic gaps in youth mental health care in San Diego. With the rise of AI, it is essential to leverage these tools to create digital health solutions that aim to address current healthcare challenges.
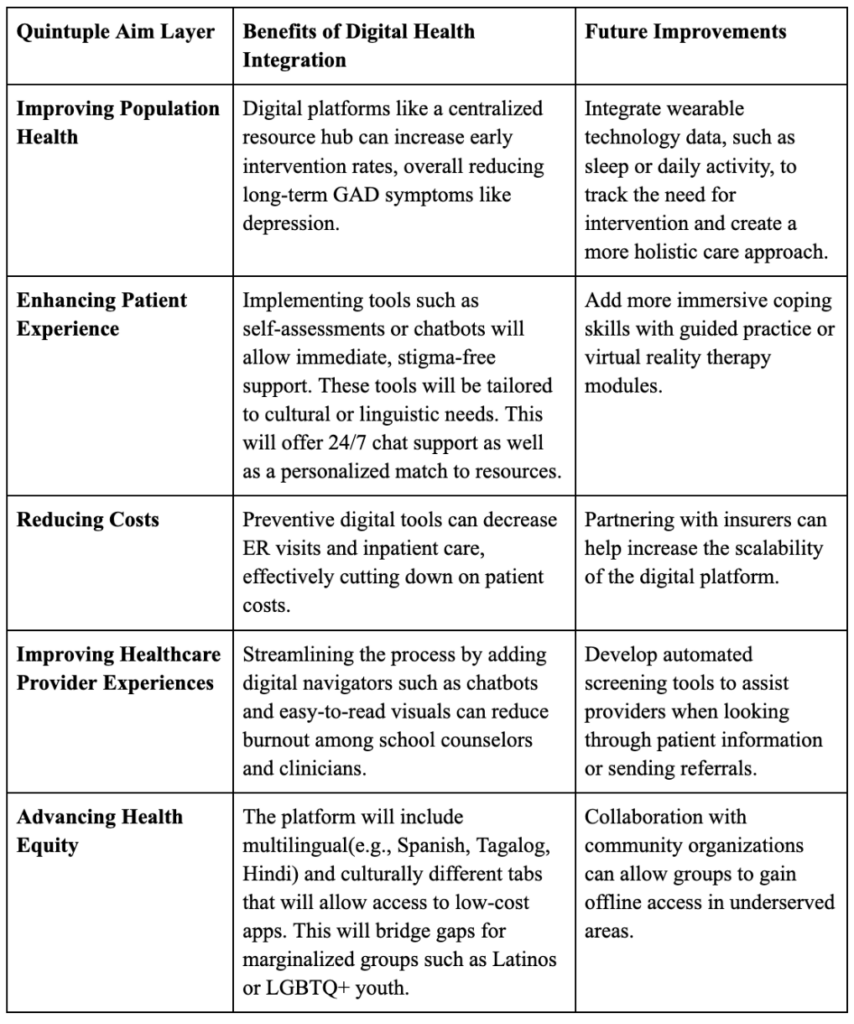
Table 2: Quintuple Aim of Healthcare
Plan of Action
The team is creating a two-pronged strategy to increase accessibility and decrease the stigma associated with mental health care to address the growing crisis of GAD among adolescents in San Diego. As part of this strategy, (1) high school students will be trained as peer “Digital Navigators” by becoming Youth Mental Health First Aid (YMHFA) certified, and (2) a digital platform that centralizes local mental health resources will be created. This strategy is aimed at San Diego Area teenagers between the ages of 13 and 18.
From Month 1 to Month 3, we plan to start the development and set up of our intervention. This will include building a culturally responsive, user-friendly website consolidating guides of mental health resources for teens in the area, as well as a feature that allows users to find mental health providers near them through filtering by age, ethnicity, and gender. We will then reach out to partner with local organizations, such as NAMI’s San Diego chapter, Project UNITY, UC San Diego, and the San Diego Unified School District, the largest public school district in the area, securing partnerships by mid/end of September. Through partnering with the school district and reaching out to other local schools, we plan to recruit 15-25 teens for YMHFA training in order to start implementing the digital navigators portion of our intervention. After finishing the website, we will get feedback from at least three of our partners before officially launching the edited version in October.
From Month 4 to Month 6, we plan to introduce our pilot program and begin implementing outreach. This begins with launching the edited version of our website and collecting user feedback from at least 50 users by the end of December. By the end of the year, we also intend to get the 15-25 students who volunteered for YMHFA training officially certified in mental health first aid so they can begin their roles as digital navigators. By the end of January, we plan to expand promotion of our website and the new digital navigators through school visits, impacting three districts (not necessarily every school in the district), with at least one of these being in an underserved community. Social media is also a crucial part of raising awareness for our program, and we aim to have at least 500 followers on a social media platform by January 2026.
From Month 7 to Month 9, we want to evaluate where we are and expand from there based on feedback. This will be done by tracking the site usage and getting more feedback from users, aiming for at least 50 new responses by the end of March. After this, April will be spent making improvements to the platform based on the feedback received, with the website fully updated by the end of the month. Finally, we will recruit 25-30 new navigators for YMHFA training in the coming months and collect feedback from at least 10 existing navigators on what to change in terms of training and implementation of the navigator system in order to ensure maximum impact.
From Month 10 to Month 12, we will focus on sustainability and long-term impact by transitioning to school-based clubs, creating chapters in at least 4 school districts in San Diego to expand outreach and ensure widespread, long-term impact. Next, we will implement a system of bi-annual Navigator check-ins, making changes to the digital navigator system after each check-in to maximize the efficacy and efficiency of the system. In addition, we plan on adding 30 new navigators per school year. This ensures sustainability by creating a system where Navigators are consistently being added and have peers who have already had experience as navigators to help them, effectively creating a self-sustaining system. We plan on continuing community outreach at this time by reaching at least 5 underserved schools in San Diego. Finally, we will annually update the website based on feedback from users – this also plays a pivotal role in ensuring sustainability by creating a platform that has accurate, up-to-date information about resources and how to access them, as well as expanding our provider database each year to give users a wider variety of options.
The target population for this intervention includes adolescents aged 13–18 living in San Diego County, with a primary focus on youth from low-income, Latino, and other ethnic minority communities. Studies have shown that Latino youth in particular experience disproportionately high rates of undiagnosed and untreated anxiety disorders due to structural barriers, stigma, and limited access to culturally sensitive care4,6. By focusing on this demographic, the intervention aims to close a critical gap in awareness, accessibility, and trust in local mental health systems. Furthermore, the efficacy of this intervention is supported by the findings of both the literature review and stakeholder perspectives. Studies show that access to culturally competent care improves the quality and accessibility of treatment for teens with anxiety27. Stakeholder consultations underscored the necessity for a centralized, easy-to-navigate digital resource that addresses the confusion teens often face when trying to find appropriate services, as well as catering to the needs of certain demographics by accommodating preferences through the filter system. Furthermore, stakeholders expressed concern regarding the lack of awareness spread to youth about available resources, which our intervention aims to solve through training teens in Mental Health First Aid to become digital navigators. This multi-modal approach ensures that awareness and accessibility are consistent and present in youth communities.
Resource Allocation:
To successfully implement this intervention, we will need funding for website development, mental health first aid training for student navigators, and outreach materials. Targeted funding sources encompass: local grants (San Diego County Behavioral Health Services or The California Endowment), university partnerships (UCSD or SDUSD mental health programs), and nonprofit collaborations (e.g., NAMI San Diego, The Trevor Project). Key personnel will include web developers (e.g., volunteer students and professionals), mental health trainers, and community liaisons to ensure access to relevant resources for diverse cultures. Training sessions can be held at schools, community centers, or virtually through conferencing software(Zoom, Google Meet, Microsoft Teams), consisting of a laptop, mental health first aid materials, and digital marketing tools.
Evaluation & Monitoring:
Effectiveness will be measured through digital engagement metrics, such as website visits or resource downloads, as well as conducted pre-and post-intervention surveys assessing users’ mental health literacy and resource accessibility. We can evaluate the efficacy through success indicators such as increased awareness of mental health resources, higher utilization of tools (measured by click-through rates), and potential reductions in self-reported GAD symptoms. Data will be collected through anonymous surveys, Google Analytics, and follow-up interviews or reviews with student navigators. For sustainability, we will teach school clubs how to maintain the platform, conduct bi-annual check-ins with community leaders, and establish a form of student organization to ensure long-term continuity.
Project UNITY Support:
Partnership with Project UNITY augments operational capacity by promoting the platform through their social media and youth networks, enabling connection with mental health advocates and potential funders, and offering guidance and targeted outreach if the project were to go further than San Diego. Additionally, a collaboration with Project UNITY could involve co-hosting workshops or integrating the platform into existing programs. This structured approach would ensure that the intervention is well-resourced, measurable, and sustainable in addressing the youth mental health needs in San Diego.
Discussion
Our intervention combines technology and peer support to address the needs of students facing mental health challenges. Our digital platform and Digital Navigators offer a more approachable and culturally relevant option, improving the chances of someone finding care that fits their needs. It is especially helpful in communities where stigma and language barriers make it hard for youth to get professional help. This model also gives students more agency over their mental health and increases trust among users. However, our approach has some limitations. One concern is maintaining the website over time since it will need ongoing technical support and funding. Another challenge is ensuring that student Navigators feel confident in their roles. They must understand their limits since they are volunteers, not trained professionals. Finally, engagement with our platform may vary based on school participation or student interest, especially if stigma around mental health remains strong in some communities. To tackle these issues, we plan to partner with local organizations, schools, and universities for ongoing support. We will also gather feedback regularly from users and Navigators to improve the platform and keep the program relevant. While our intervention is not a complete solution to youth mental health, it helps by making existing resources easier to access and by building a peer support system that can grow over time.
This solution utilizes digital health to address multiple components of the Quintuple Aim. By providing a user-friendly website with personalized filters that allow individuals to find providers based on gender, age, and ethnicity, we enhance the patient experience and promote health equity by making culturally and demographically competent care seem less out of reach, as it is all consolidated in one place. This improved access supports population health by promoting early intervention and better management of GAD within the community. In turn, by improving the process of accessing appropriate resources, our intervention has the potential to reduce healthcare costs associated with unnecessary or delayed care as a result of worsened, untreated anxiety. Training teens as digital navigators adds a peer support layer that improves digital literacy and engagement, which not only enhances patient experience but also supports care team well-being by reducing navigation burdens on providers, relieving some of the backlog in the healthcare system, and allowing professionals to focus on the most pressing cases.
Conclusion
GAD in adolescents has become a significant public health concern, with prevalence rates increasing substantially in recent years. An alarming number of teens experience emotional distress but are unable to access appropriate treatment due to stigma, limited availability of services, and cultural barriers. In San Diego County specifically, approximately 25% of adolescents aged 13 to 18 are affected by anxiety, with Latino youth and female students reporting disproportionately high levels of emotional stress15. Our proposed intervention seeks to address these challenges by enhancing access to mental health care for adolescents in San Diego, with a particular emphasis on those facing socioeconomic disadvantages and cultural obstacles. The key components of our intervention include the development of a culturally responsive mental health website and the implementation of a peer-led support system through the training of students in Youth Mental Health First Aid. These students will assist their peers in navigating local mental health resources tailored to their linguistic, cultural, and personal needs. By establishing a sustainable model that integrates digital tools and empowers youth as mental health advocates, this initiative aims to promote more personalized, inclusive, and equitable care. Future research should further investigate the most significant barriers contributing to the underutilization of GAD resources among adolescents. Additionally, studies should explore the most effective strategies for overcoming these barriers and examine preventative approaches to ensure that future interventions are proactive rather than reactive.
References
- Generalized Anxiety Disorder (GAD). Boston Children’s Hospital. Available at: https://www.childrenshospital.org/conditions-treatments/generalized-anxiety-disorder-gad.
- Centers for Disease Control and Prevention. Data and statistics on children’s mental health. Children’s Mental Health (2025). Available at: https://www.cdc.gov/children-mental-health/data-research/index.html.
- Greenberg, P. E., Fournier, A.-A., Sisitsky, T., Pike, C. T. & Kessler, R. C. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J. Clin. Psychiatry 76, 155–162 (2015).
- Merikangas, K. R. et al. Service utilization for lifetime mental disorders in U.S. adolescents: Results of the National Comorbidity Survey–Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 50, 32–45 (2011).
- Vargas, N., Anderson, J., Lawson-Remer, T., Steppe, M. M. & Desmond, J. County of San Diego Board of Supervisors.
- Ahad, A. A. et al. Understanding and addressing mental health stigma across cultures for improving psychiatric care: A narrative review. Cureus 15 (2023).
- Zehrung, R., Hu, D., Guo, Y., Zheng, K. & Chen, Y. Investigating the effects of housing instability on depression, anxiety, and mental health treatment in childhood and adolescence. AMIA Annu. Symp. Proc. 2024, 1303–1312 (2025).
- Anderson, D. et al. The Healthy Minds, Thriving Kids Project: Educator perspectives on relevance and potential impact of a mental health skill building program. PLOS ONE 20, e0305450 (2025).
- Dindo, L. N., Recober, A., Haddad, R. & Calarge, C. A. Comorbidity of migraine, major depressive disorder, and generalized anxiety disorder in adolescents and young adults. Int. J. Behav. Med. 24, 528–534 (2017).
- Aguilar Silvan, Y., Fortuna, L. R., Spencer, A. E. & Ng, L. C. Engagement in child psychiatry department appointments: An analysis of electronic medical records in one safety-net hospital in New England, USA. J. Health Serv. Res. Policy 30, 79–88 (2025).
- von der Embse, N., Jester, D., Roy, D. & Post, J. Test anxiety effects, predictors, and correlates: A 30-year meta-analytic review. J. Affect. Disord. 227, 483–493 (2018).
- Liu, C. H. et al. The prevalence and predictors of mental health diagnoses and suicide among U.S. college students: Implications for addressing disparities in service use. Depress. Anxiety (2019). https://doi.org/10.1002/da.22830.
- Smith, S. N. et al. Student mental health outcomes of a clustered SMART for developing an adaptive implementation strategy to support school-based CBT delivery. J. Affect. Disord. 367, 399–407 (2024).
- Rady Children’s seeing 25% increase in mental health ER visits. KPBS Public Media (2021). Available at: https://www.kpbs.org/news/midday-edition/2021/06/09/rady-childrens-seeing-25-increase-mental-health-em.
- MHSA rotating report 2020: Depression in youth.
- Recent trends in mental health and substance use concerns among adolescents. KFF. Available at: https://www.kff.org/mental-health/recent-trends-in-mental-health-and-substance-use-concerns-among-adolescents/.
- Smythe, J., Jimenez, M. & Romain, D. Research design collaborators.
- March 2024 data update.
- Bögels, S. M. & Brechman-Toussaint, M. L. Family issues in child anxiety: Attachment, family functioning, parental rearing and beliefs. Clin. Psychol. Rev. 26, 834–856 (2006).
- McLeod, B. D., Wood, J. J. & Weisz, J. R. Examining the association between parenting and childhood anxiety: A meta-analysis. Clin. Psychol. Rev. 27, 155–172 (2007).
- Elhai, J. D. et al. Testing whether posttraumatic stress disorder and major depressive disorder are similar or unique constructs. J. Anxiety Disord. 25, 404–410 (2011).
- Va, S. New report details student mental health crisis in California. ACLU California Action (2022). Available at: https://aclucalaction.org/2022/01/new-report-details-student-mental-health-crisis-in-california/.
- School counselor roles & ratios. American School Counselor Association. Available at: https://www.schoolcounselor.org/About-School-Counseling/School-Counselor-Roles-Ratios.
- Parks master plan. City of San Diego Official Website. Available at: https://www.sandiego.gov/parks-for-all-of-us.
- Youth at the center.
- 2022–23 San Diego report DMC ODS.
- Alegria, M., Atkins, M., Farmer, E., Slaton, E. & Stelk, W. One size does not fit all: Taking diversity, culture and context seriously. Adm. Policy Ment. Health Ment. Health Serv. Res. 37, 48–60 (2010).
Related Posts

Risk of Death Among Recently Released Inmates
Figure 1: While healthcare inequity is certainly an issue while...
Read More
Concierge Medicine Could Reduce Senior Health Inequities in Illinois
This publication is in proud partnership with Project UNITY’s Catalyst Academy 2023...
Read More
Understanding the Social Factors Affecting Cancer Therapy
Cover Image: A patient being prepared for radiation therapy. (Source:...
Read More
Investigating Obstructive Sleep Apnea (OSA) in African and Latin Americans from Chicago
This publication is in proud partnership with Project UNITY’s Catalyst Academy 2024...
Read More
How Many Humans Does it Take to Host a Planet?
Figure 1: This is an artist’s rendering of a potential...
Read More
Mind Missing Out? Fear of Missing Out and the Brain
Figure: A person scrolling through news articles on their smartphone....
Read MoreDarius Dastur, Mishal Ali, Harshitha Ezhilarasan, Hasan Khan, Aaron Akasala