Abstract
Background: Coronary Artery Disease (CAD) is the leading cause of mortality in the US. There is a lack of awareness on how to prevent CAD, as well as risk factors and social determinants of health (SDOH) that increase susceptibility to it, especially for the African Americans population. Objectives: The purpose of this review is to analyze and synthesize the various factors that contribute to the susceptibility of CAD within the African American community in Illinois and the U.S more broadly. By recognizing these key components, an effective public health intervention can be designed and implemented to minimize the effects of CAD. Methods: This review was conducted using PubMed, American Heart Association Journals, the Center for Disease Control and Prevention, and other scholarly sources relevant to the keywords. Over 110 pieces of literature were reviewed and synthesized. Results: The African American community is at the highest risk of CAD within Illinois and the United States due to biological, genetic, cultural, behavioral, and socioeconomic reasons. This includes hypertension, smoking, family history, segregation, redlining, and lack of quality healthcare in African American communities. Conclusion: Due to the various SDOH concerning African American communities, African American individuals are unable to receive the equitable quality healthcare needed to care for CAD, especially in Illinois. It is imperative for individuals to proactively initiate healthcare interventions that provide essential resources and education to empower the African American community.
Keywords: Coronary Artery Disease, African Americans, Social Determinants of Health, Prevalence and Risk Factors of Cardiovascular Diseases, Health Implications, Cardiovascular Health Interventions in Illinois.
Introduction
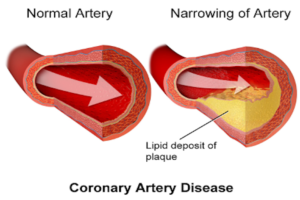
Coronary artery disease (CAD) is defined by plaque buildup in the coronary arteries, narrowing blood vessels and reduced flow of blood to the heart and body2. Although Cardiovascular Diseases (CVDs) have impacted the U.S. and Illinois greatly, CAD in particular has had the most detrimental impacts both nationwide and locally. African American individuals statistically have the highest mortality rate from CAD in the United States5, making it a significant public health issue. It is necessary to ensure that the large African American population in Illinois is protected from the effects of CAD, as African Americans compose 14.7% of the population, a large percentage compared to other states within the US8. From our Literature Review and Evidence-Based Research Review, our team was able to understand how and why the African American population is so heavily impacted by CAD: the various SDOH that affect African Americans, such as a relative lack of education, and their vulnerability to risk factors influenced by genetics and lifestyle choices. Although there are state-level initiatives within Illinois run the government and other organizations, it is imperative that more interventions are created to address the disparities that disproportionately affect the African American community.
This review analyzed over 110 existing articles through avenues such as PubMed, ScienceDirect, and Google Scholar to determine potential connections between CAD within the U.S. and Illinois, and the African American population. Our team engaged in discussion with representatives from the American Heart Association and Heart Smart EKG to create a plan of action to combat risk factors and SDOH specific to Illinois.
Across the United States, the African American community faces the highest rates of CAD. 20 million African American individuals in the U.S. have been diagnosed with CAD, and every year, African Americans account for 100,000 CAD deaths3. These numbers demonstrate the urgent need to address the various risk factors that contribute to these high death rates.
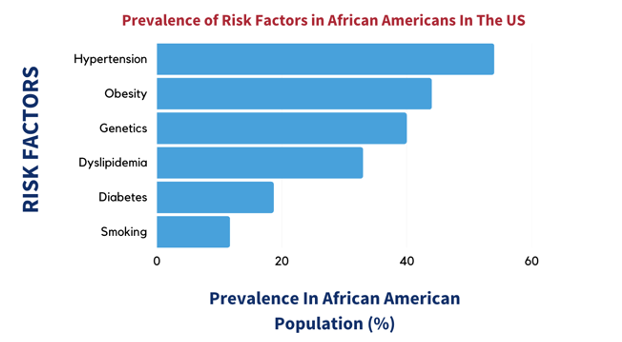
Genetic factors play an important role in increasing susceptibility to CAD. Certain genetic variants that increase the likelihood of dyslipidemia (high levels of cholesterol or fats) and hypertension (high blood pressure) are more prevalent in African American populations than other populations9. Cultural elements also factor into higher rates of CAD, such as traditional eating habits – for example, eating lots of ‘soul food’ which has high contents of fats and sugars – as well as attitudes towards exercise1.
Fortunately, the impacts can be mitigated. 90% of CAD diagnoses can be prevented through lifestyle changes such as improved nutrition and frequent exercise. But making these changes depends on knowledge of the various risk factors and how they can contribute to CAD6. A nationwide effort to spread awareness of these risk factors would be helpful for suppressing the high levels of CAD within the African American community.