
This publication is produced in partnership with Project UNITY’s Catalyst Academy Class of 2025, a student public health research and education program.

Abstract
Substance Use Disorder (SUD) is a brain disorder characterized by the persistent use of drugs despite detrimental consequences to oneself or others (NIDA, 2020). SUD develops through a combination of genetic predisposition, environmental factors, adverse childhood experiences (ACEs), and mental health conditions (Felitti et al., 1998; Compton & Volkow, 2006). In 2022, approximately one in six Americans aged 12 and older were affected by SUD (SAMHSA, 2023). Declared as a public health emergency in 2017, the opioid crisis has been renewed through 2025, making it an essential topic to target through a public health lens (U.S. Department of Health and Human Services, 2025). To investigate how ACEs in dysfunctional homes influence SUD at the local and national level and to design an evidence-based solution for young adults with SUD in Richmond, Virginia, 45 articles from PubMed, the Center for Disease Control, the Substance Abuse and Mental Health Services Administration, and other relevant sources were analyzed, focusing on substance abuse, ACEs, and their intersection. Interviews were conducted with a board-certified Addiction Medicine and Family Medicine specialist and a board-certified Pediatric Psychiatrist to gain insights to inform the proposed plan of action. Young adults emerged as the most vulnerable population to SUD. Economic stability, access to education, access to healthcare, and environmental factors play a significant role in developing SUDs. Most existing interventions lack personalized, adaptive care and early intervention. This report outlines a comprehensive intervention plan that addresses gaps in current treatment by integrating virtual reality into substance abuse therapy in Richmond, Virginia. This approach aims to address the root causes of SUD and has the potential to be scaled for broader implementation at the national and global levels.
Keywords: Public health intervention; substance use disorder; adverse childhood experiences; virtual reality; artificial intelligence
Introduction
Childhood trauma is widely recognized as a major contributor to mental and behavioral health concerns that persist into adulthood, making this a critical focus of public health efforts. Experiences of early adversity, better known as Adverse Childhood Experiences (ACEs), include physical, sexual, and emotional abuse, neglect, exposure to domestic conflict, and chronic instability within the household (Felitti et al., 1998). These events disrupt healthy childhood development by exposing individuals to prolonged stress, which has been shown to alter brain networks, impair emotional regulation, and create coping behaviors that often persist across the lifespan (Sinha, 2008). A particularly harmful consequence of these environments is parentification, the phenomenon in which children assume adult caregiving responsibilities to maintain family functioning. Over time, this role reversal places a heavy emotional burden on children, thereby depriving them of normal developmental experiences. The chronic stress and emotional suppression that result often set the stage for substance use in adolescence and early adulthood as a means of coping (Hooper et al., 2011; Chase, 1999). This direct link between unresolved childhood adversity and later self-medication underscores why Substance Use Disorders (SUDs)—medical conditions defined by the persistent use of drugs or alcohol despite harm—are so strongly associated with ACEs and parentification (Hooper et al., 2011). Further, SUDs can lead to severe health problems, such as liver and cardiovascular disease, mental illness, overdose, and premature death (Compton & Volkow, 2006). The social effects are equally damaging, as untreated SUDs strain relationships, disrupt families, and weaken community well-being. Economically, these disorders place a heavy burden on public resources. In 2022 alone, more than 48 million Americans aged 12 and older were affected by SUDs, contributing to billions of dollars in healthcare costs, loss of productivity, and criminal justice expenses (American Addiction Centers, 2023; National Institute on Drug Abuse, 2023a).
Therefore, this paper focuses on the intersection of childhood trauma, parentification, and SUDs, with particular emphasis on Richmond, Virginia—a city disproportionately affected by the opioid crisis in recent years (Virginia Department of Health, 2023). The primary objective is threefold: first, to investigate how early trauma and dysfunctional household dynamics contribute to the development of SUDs in young adults; second, to identify the social determinants of health that intensify these risks at both local and national levels; and third, to design an evidence-based intervention to address these challenges.
The Importance of a Public Health Lens
Substance abuse must be addressed through a public health framework because it is not only a personal or clinical issue, but a multidimensional crisis rooted in structural, social, and environmental contexts. At the individual level, factors such as genetic predisposition, chronic stress, and early childhood trauma, particularly Adverse Childhood Experiences (ACEs), increase vulnerability to substance use and relapse (Felitti et al., 1998). Even those who wish to engage in protective behaviors may lack access to health education, transportation, or affordable wellness resources. Individuals raised in environments shaped by poverty, violence, or neglect often experience compounded risk that traditional clinical care does not fully address (Marmot, 2005). Interpersonal dynamics further intensify this risk: stigma and fear of rejection from family, peers, or religious communities often deter individuals from seeking help, even when services are available. Thus, this social stigma becomes a powerful barrier to treatment initiation and retention (Livingston et al., 2012), particularly among marginalized populations already facing structural discrimination.
Organizational and community-level barriers additionally entrench these disparities. In rural and underserved areas, clinics and recovery centers may be under-resourced or geographically inaccessible, leading to delayed diagnoses, inadequate care, or forced reliance on emergency services (SAMHSA, 2020). For instance, insurance restrictions can limit access to culturally competent providers, while bureaucratic hurdles disproportionately affect low-income individuals and essential workers who cannot afford to miss work for appointments. At the community level, underfunded schools may lack mental health counselors or substance use prevention programs, leaving youth to navigate trauma without support. In these settings, substance use often becomes a coping mechanism rather than a choice. At the policy level, generalized federal responses frequently overlook local realities. For instance, funding may bypass high-need areas or fail to support trauma-informed and community-based care models proven effective in reducing substance use disparities (Compton & Volkow, 2006). Thus, recognizing these interconnected layers of risk demonstrates that addressing substance use disorders requires coordinated solutions that extend beyond clinical treatment alone.
Methods
To better understand the link between early trauma and substance abuse in emerging adults, particularly within the Richmond, Virginia context, scholarly databases such as PubMed and Google Scholar, as well as government and state health resources including the Centers for Disease Control and Prevention (CDC), the Substance Abuse and Mental Health Services Administration (SAMHSA), and the Virginia Department of Health, were consulted. Sources that examined adolescent substance use through the lens of mental health, family instability, and ACEs were prioritized. Particular attention was paid to articles that highlighted barriers to care and structural inequities that shape health outcomes for youth in urban, under-resourced areas.Richmond-specific sources and community-level data were emphasized to ensure that the analysis was locally grounded and responsive to the unique needs of the city. Articles that were narrowly biomedical in focus, did not address behavioral or structural determinants, or were unrelated to U.S. or comparable contexts were excluded from detailed review. In total, 59 articles were thoroughly reviewed across these sources.
To supplement the literature, stakeholder interviews were conducted with local professionals who regularly interact with adolescents affected by substance use. Stakeholders were selected based on their expertise in mental health, addiction medicine, pharmacy, social work, and community health programming, while prioritizing those who worked directly within Richmond or with a similar population. Three stakeholders, including a pharmacist, an addiction medicine specialist, and a psychiatrist, participated in interviews conducted over Zoom, which were recorded with consent and transcribed for thematic analysis. Key questions explored trauma-informed care systems, stigma-related treatment avoidance, and gaps in existing recovery infrastructure. Insights from these interviews were then synthesized into a coherent summary document for analysis.
To develop the Plan of Action, results from the literature review, such as the clear connection between Adverse Childhood Experiences (ACEs), unresolved trauma, and later substance abuse, was considered. The Plan of Action is focused on supporting young adults aged 18–25 in Richmond who have been affected by ACEs by introducing a trauma-informed Virtual Reality (VR) therapy combined with education and community outreach. The measures would be well-suited to the target population, as current care systems lack personalized interventions that address trauma early, and many existing programs do not integrate modern technology into treatment. The VR-based approach would include interactive simulations guided by mental health professionals that teach emotional regulation, boundary setting, and coping skills.
Literature Review
Substance abuse remains one of the most complex and persistent public health crises in the United States. In 2022 alone, approximately 48.5 million people aged 12 and older were diagnosed with a substance use disorder (SUD), thereby highlighting the expansive and enduring nature of the issue (American Addiction Centers, 2023). While substance use has long posed a public health concern, the emergence of the opioid epidemic has exacerbated health disparities and introduced new, more lethal threats. Between 2000 and 2019, overdose deaths increased by over 255%, with synthetic opioids like fentanyl responsible for numerous fatalities (National Center for Drug Abuse Statistics, 2023). Most critically, young adults aged 18 to 25 consistently show the highest rates of illicit drug use and prescription drug misuse, often compounded by untreated trauma and structural disadvantage (National Institute on Drug Abuse, 2023). National data also indicate that SUD disproportionately affects individuals living in rural communities, those with low income, Black and Native American populations, and individuals with a history of ACEs (SAMHSA, 2020; Compton & Volkow, 2006), highlighting the unequal burden of the crisis. Among the most insidious risk factors is childhood parentification: a form of role reversal where children assume caregiving responsibilities in the place of parents or siblings. Research increasingly links parentification to long-term emotional distress, identity confusion, and maladaptive coping behaviors such as substance use (Hooper et al., 2011).
Furthermore, social determinants of health, as outlined in the Healthy People 2030 framework, are inextricably tied to the onset and outcomes of SUD; for instance, low educational attainment, reduced health literacy, and lack of access to culturally competent mental health services lead to delayed treatment, while exposure to unsafe neighborhoods, community violence, and targeted marketing of addictive substances further reinforce risk patterns (Compton & Volkow, 2006; SAMHSA, 2020). Accordingly, for individuals raised in dysfunctional homes, these compounding determinants create environments where the path to addiction is predictable and structurally embedded.
Our research team consists of members from Richmond, Virginia, and Cincinnati, and the data reports the most disproportionate findings in Richmond. As of 2023, Richmond has witnessed a 350% increase in overdose deaths since 2019, compared to the national average of an estimated 50% increase over the same period (Virginia Department of Health, 2023). Richmond recorded a staggering 297 overdose deaths in 2023 alone, five times the national average. Public housing communities such as Gilpin Court, Mosby Court, and Whitcomb Court report some of the highest overdose prevalence and EMS (Emergency Medical Services) call rates in the state, disproportionately affecting Black and low-income residents. Specifically, youth in these communities are raised in households affected by substance use, incarceration, and systemic neglect, making Richmond a uniquely urgent site for intervention.
At the individual level, poverty and chronic stress serve as powerful predictors of future substance use. Richmond’s poverty rate stands at nearly 27%, significantly higher than the national average (U.S. Census Bureau, 2023). Youth raised in poverty are more likely to experience food insecurity, exposure to violence, and unstable housing—conditions that activate toxic stress responses and damage long-term mental and physical health. In parallel, parentified youth often suppress their own needs and internalize a sense of hyper-responsibility, which impairs emotional regulation and self-concept. In addition, limited access to healthy foods, consistent transportation, and quality education leave these individuals with fewer tools to manage stress adaptively. Research shows that individuals from low-income backgrounds are more likely to delay care, underestimate the risks of drug use, and lack access to early behavioral health interventions (Compton et al., 2007).
Interpersonal dynamics also play a critical role in shaping substance use risk and recovery pathways. In many of Richmond’s most impacted neighborhoods, family structures are frequently disrupted by incarceration or financial instability, contributing to child-parentification, emotional burnout, internalization of guilt and shame, and later SUD (Hooper et al., 2011). Peer influences during adolescence further compound the risk. In the absence of protective relationships, many youth seek connection through peer groups where substance use is normalized. Conversely, those with healthy peer support systems and positive adult role models are more likely to develop resilience and seek healthy coping strategies (Prinstein & Dodge, 2008). Many underserved Richmond neighborhoods lack structured opportunities for mentorship or peer-led recovery support, leaving youth especially vulnerable during transitional life stages.
Organizational systems play a major role in whether at-risk youth are identified, supported, and referred to treatment. Local efforts in Richmond, such as the Opioid Response Task Force and harm reduction vending machines, represent promising steps forward (RVA Human Services, 2023). However, although substance use education is provided across all public schools in Richmond, implementation is rather inconsistent, and many low-income schools lack the necessary staffing or infrastructure to deliver trauma-informed care. For many students, schools are the only touchpoint with a mental health professional, yet services are often overstretched or entirely absent (ChildSavers, 2023). Outside of school, healthcare access remains uneven, particularly for young adults without stable insurance or transportation. Cultural mismatches between providers and patients and a lack of trauma-informed training further deter participation. In the workforce, entry-level and essential jobs, frequently held by individuals from low-income or marginalized communities, rarely offer paid leave or behavioral health benefits, making it logistically difficult to attend treatment appointments or seek support (Bureau of Labor Statistics, 2022).
Likewise, community environments can either buffer against or exacerbate substance use risk. Richmond is home to organizations including the McShin Foundation and the Richmond Behavioral Health Authority (RBHA), which offer naloxone distribution, peer mentorship, residential treatment, and harm reduction education (VCU News, 2023). While these resources are invaluable, their capacity often fails to meet the scale of the crisis. Many programs report waitlists or staffing shortages. Persistent stigma surrounding addiction and mental health continues to discourage care-seeking, particularly among many young men, youth of color, and parentified youth.
Policy remains a powerful lever in either enabling or hindering access to care. National initiatives such as the Mental Health Parity and Addiction Equity Act and the Affordable Care Act have expanded access to behavioral health services, which have been particularly effective in increasing treatment participation statewide (Beronio et al., 2014; Virginia Medicaid, 2020). Yet, gaps persist. School-based mental health programming remains underfunded, and community-based prevention lacks continuity. Furthermore, policies rarely account for trauma histories like parentification or childhood emotional neglect, despite their clear links to later addiction. Thus, intervening at this intersection, where early caregiving trauma meets system-level failure, is therefore essential for long-term, equitable change.
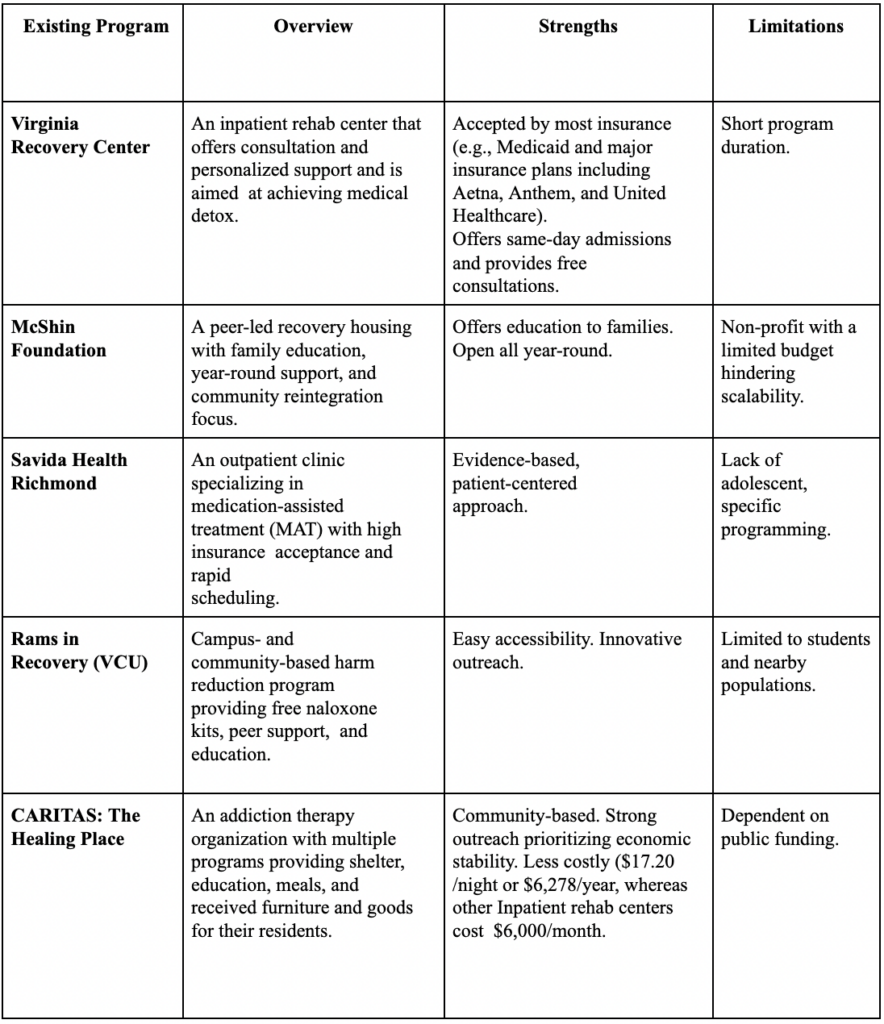
Table 1: Overview of Substance Abuse Programs for Youth and Young Adults in Richmond, VA
Stakeholder Perspectives
Two key stakeholders, Dr. Vincent Nardone, a board-certified Addiction Medicine and Family Medicine specialist and Medical Director of Foundation Medical Group, and Dr. Ankita Zutshi, a board-certified pediatric psychiatrist, were interviewed. Together, their perspectives highlighted the complex drivers of substance use, the opioid epidemic, and adolescent mental health challenges.
Dr. Nardone explained that the opioid epidemic stems largely from the overprescription of opioids as pain medications. For decades, these drugs were promoted as safe and minimally addictive, which, combined with the U.S. healthcare system’s emphasis on pain management and patient satisfaction, led to widespread and high-dose use. He also noted that stigma is a major barrier to recovery: in his Utah practice, the predominantly Mormon community views addiction as a moral failing rather than a medical condition. Reframing SUD as a chronic medical disease, he argued, improves patient outcomes and willingness to seek treatment. Beyond stigma, Dr. Nardone highlighted how poverty, housing instability, lack of healthcare access, trauma, and isolation, factors that worsened during the COVID-19 pandemic, also serve as social determinants preventing people from engaging in care.
On the other hand, Dr. Zutshi focused on adolescent mental health, describing how generational cycles of abuse and substance use perpetuate unhealthy coping behaviors in children. Parents struggling with their own crises often delay treatment for themselves and are less able to recognize problems in their children. She also emphasized cultural and structural barriers, such as the deep distrust of healthcare among African Americans due to historic and ongoing discrimination (Pew Research Center), as well as the rural-urban divide in access to care. Individuals in rural communities tend to experience greater poverty, have limited health insurance, and reduced availability of specialists; in fact, 65% of rural counties lack a psychiatrist (Andrilla et al., 2018; CDC, 2024). As a potential solution, Dr. Zutshi suggested that digital health platforms and AI-driven technologies, such as telepsychiatry, remote monitoring, and virtual support, could expand mental health care access in underserved areas.
Digital Health Solutions
The Quintuple Aim framework, which emphasizes improving population health, enhancing patient experience, reducing costs, improving provider experiences, and advancing health equity, offers a powerful foundation for reimagining approaches to substance abuse, particularly in emerging adults affected by parentification in Richmond (Berwick et al., 2008; Nundy et al., 2022). Digital health technologies have substantial potential in improving population health by enabling early identification of parentified youth before patterns of substance use become entrenched. Moreover, digital health interventions can dramatically enhance patient experience for emerging adults navigating substance abuse and unresolved family trauma through virtual visits and telehealth services, tools which provide confidential, judgment-free environments for individuals with a fear of stigma or family obligations (SAHMSA, 2023).
From a systems perspective, digital health solutions also play a pivotal role in reducing healthcare costs by minimizing the need for emergency department visits and inpatient admissions, thereby shifting focus to early intervention and continuous digital support. In parallel, these technologies improve healthcare provider experiences by streamlining workflows and reducing administrative burdens (Shanafelt & Noseworthy, 2017). Critically, digital health solutions advance health equity by bridging longstanding structural gaps in care access. Emerging adults from dysfunctional, low-income households in Richmond often face compounded barriers, including a lack of transportation, unstable housing, and cultural or language differences that deter engagement with seeking traditional services. In this sense, telehealth and mobile outreach solutions directly mitigate these challenges by delivering services in familiar, accessible environments (Nundy et al., 2022; SAMHSA, 2023).
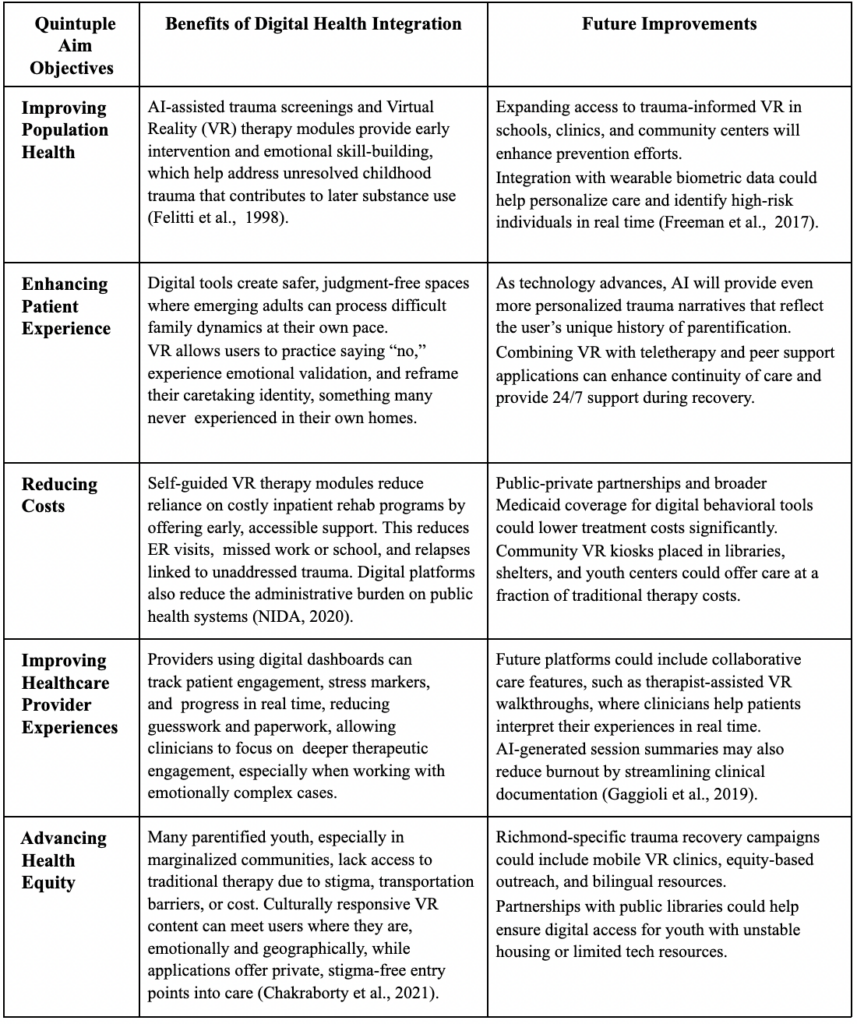
Table 2: Quintuple Aim of Healthcare
Plan of Action
The plan integrates AI-personalized Virtual Reality (VR) therapy with community education and engagement, while also providing early intervention tools to support trauma recovery among individuals (18–25) at risk of developing SUDs, particularly within under-resourced communities. Organized around the Quintuple Aim framework, this intervention will improve access to mental health care, enhance engagement through immersive and personalized VR tools, reduce long-term healthcare costs by offering scalable preventive therapy, support clinicians through integrated progress monitoring, and promote equity by prioritizing Black and Hispanic/Latino populations in Greater Richmond affected by generational trauma and the opioid crisis.
The proposed plan of action would begin in Month 1 with the co-design and prototyping of the VR solution. A multidisciplinary team will be assembled, including addiction medicine specialists, trauma-informed psychiatrists, AI/VR developers, and behavioral scientists. This team will partner with a VR company, such as BehaVR, to co-develop interactive, immersive modules, starting with a prototype “re-parenting room,” which offers guided exposure therapy to help users practice boundary setting, emotional regulation, and distress tolerance. The design phase draws on evidence from the literature demonstrating that trauma-focused, skills-based therapy, and resilience-building interventions are effective in mitigating the long-term impacts of ACEs on substance use (Maples-Keller et al., 2017; Compton & Volkow, 2006).
In Month 2, grant applications will be drafted and submitted to funders such as the National Institute of Mental Health (NIMH), with budget proposals that detail hardware costs and staffing and community rollout timelines. The team will begin community outreach in the Richmond community through tabling at local health fairs and presenting at harm reduction centers. These events will feature short, animated videos that walk viewers through the VR experience, followed by a Q&A session with clinicians and behavioral scientists. Community feedback will be gathered through post-event surveys and listening sessions to understand perceived benefits, barriers, and potential user concerns. Additionally, recruitment for a small pilot cohort will begin with a QR code that links to a brief screening form assessing trauma history and digital literacy.
In Month 3, early-stage VR kiosks will be installed in locations including outpatient clinics and peer recovery centers. These kiosks will house the prototype modules, allowing selected individuals to engage in brief sessions focused on basic emotional regulation and stress management techniques. Users will first complete a guided onboarding tutorial with a trained peer recovery specialist. To integrate mental and physical health supports, micro-kiosks offering naltrexone, harm reduction resources, and psychoeducational materials on ACEs will be installed nearby. Posters explaining VR and trauma will be displayed to reduce skepticism and encourage engagement, aligning with Dr. Zutshi’s emphasis on leveraging digital tools to bridge geographic and cultural access gaps in behavioral health (Patel et al., 2022).
In Month 4, the project will launch a companion mobile app designed to support personalization and progress tracking. Upon downloading the app, users will be invited to complete a trauma-informed intake survey that helps match them with curated VR scenarios aligned with their personal histories (e.g., bullying, neglect, domestic violence). The app will include audio journaling features, session reminders, and daily mood check-ins. Meanwhile, individuals with lived experience will be engaged to co-create narrative content for the VR world, either through storytelling circles or confidential one-on-one interviews with digital ethnographers. These stories will ensure the VR environment reflects authentic healing journeys and fosters emotional validation.
In Month 5, family and community integration will be introduced. With user consent, this phase will bring in family members to participate in modules that educate them on how to support trauma recovery. For instance, caregivers may watch a VR simulation demonstrating what PTSD triggers look like in daily life or participate in modules that role-play healthier communication strategies.
From Month 6 to Month 7, the focus will shift to policy engagement and biometric integration. In January, a legislative and payer brief will be drafted, showcasing early program metrics, such as reductions in self-reported cravings, improved emotional regulation, and increased attendance in counseling. Meetings will be scheduled with representatives from the Virginia Department of Behavioral Health and Developmental Services and Medicaid Managed Care plans to discuss coverage for VR headsets as part of outpatient treatment. In February, biometric tracking through wearable devices (such as heart rate variability sensors) will be piloted with a cohort of users. These devices will help detect elevated stress responses and prompt the app to recommend soothing modules, breathing exercises, or the option to connect with a therapist through integrated telehealth support.
In Month 8, the program will begin community-driven content creation. Thematic events, such as “Healing from Bullying” or “Coping with Parental Addiction,” will be held at locations including community centers and public parks, where users and allies can gather for storytelling circles, art therapy, and wellness picnics to destigmatize trauma, foster peer connections, and strengthen community resilience.
In Month 9, the intervention will undergo its first formal mid-year evaluation. Surveys will be distributed through the app to assess cultural sensitivity, ease of use, and perceived impact. Clinicians will review biometric and engagement data to determine patterns in usage and relapse risk. Focus groups will be facilitated with participants and staff to further inform program refinement. Using the NASSS (Non-adoption, Abandonment, Scale-up, Spread, and Sustainability) framework, implementation scientists will identify barriers to adoption and flag areas where adaptations are required. This approach ensures that complex digital health interventions can be effectively implemented and sustained in real-world settings (Greenhalgh et al., 2017).
From Month 10 to Month 11, the program will expand across the Greater Richmond area. In May, additional VR kiosks and pods will be installed in emergency departments, probation offices, and YMCA branches. Community ambassadors who completed the initial intervention will be trained to facilitate peer support groups and introduce new participants to the program. In June, lessons learned will be compiled into a digital replication toolkit for other cities. By July, long-term app features, including monthly challenges, progress reports, and personalized content recommendations, will be fully deployed.
In Month 12, a comprehensive outcome analysis will be conducted. Quantitative metrics (e.g., session completion rates, relapse reports, heart rate variability) will be triangulated with qualitative insights from user narratives and clinician notes. Findings will be synthesized into a final report shared with funders, policymakers, and public health leaders.
Discussion
A key strength of our intervention is its integration of AI with virtual reality (VR) to address mental health challenges among youth with Adverse Childhood Experiences (ACEs). While VR has been applied previously for exposure therapy and PTSD treatment (Maples-Keller et al., 2017), few interventions combine adaptive AI with diagnostic capabilities to provide individual-centered care for adolescents with ACEs (Schickedanz et al., 2018). An additional strength is the focus on clinical integration. Providers can assign targeted simulations and track usage metrics, enabling identification of symptom patterns, emotional triggers, and coping strategies. This structure closes the feedback loop between therapist and patient while enhancing care coordination (Topol, 2019; Luxton et al., 2015).
Despite these strengths, several limitations must be acknowledged. Although short-term improvements in PTSD and anxiety symptoms have been documented (Geraets et al., 2021), the long-term efficacy and behavioral durability of this technology remains under-researched. To address this limitation, the proposed intervention implements a longitudinal evaluation component with opt-in follow-up surveys and periodic progress check-ins embedded within the software. Additionally, the use of AI and digital diagnostics raises concerns about privacy, data security, and regulatory compliance, particularly when working with minors. To mitigate risks, this intervention will adhere to the HIPAA and COPPA regulations, employ end-to-end encryption, and undergo routine third-party audits to maintain legal and ethical data stewardship (Cuggia & Combes, 2019).
Overall, our proposal addresses the barriers to recovery such as stigma and affordability with an accessible AI-personalized virtual reality solution, combined with community engagement and education, it provides a promising solution with trauma-informed care.
Concluding Remarks
Substance abuse remains one of the most pressing public health crises, affecting millions worldwide and leaving lasting effects. Unfortunately, despite available treatment programs, barriers such as stigma, affordability, and lack of trauma-informed care prevent equitable access. Thus, our proposed plan addresses these gaps through an AI-personalized virtual reality (VR) therapy paired with education and community outreach. These strategies can transform recovery and reduce the burden of substance use disorders across the country. Future research should focus on validating long-term outcomes, ensuring ethical AI use, and expanding accessibility so that personalized VR-based interventions can be safely and equitably integrated into existing addiction treatment systems.
Author’s Contributions
There were three authors and one mentor. All authors contributed equally to the Literature Review, Plan of Action, and References. Tanusiya Debnath authored the Abstract, Keywords, Conclusion, and her portion of the stakeholder interview with Dr. Vincent Nardone, an Addiction Medicine Specialist. Ananya Agarwal completed her portion of the stakeholder section after interviewing Dr. Ankita Zutshi, a Psychiatrist at Cincinnati Children’s Hospital, and contributed to the Introduction. Sanya Joshi authored the Discussion. Other sections, including the Quintuple Aim Model, Digital Health Solutions, Strengths and Limitations, and Methods, were developed collaboratively by all authors. Soha Khoso provided feedback, helped edit and format, and mentored all authors throughout the writing process to ensure a high-quality paper.
References
- National Institute on Drug Abuse. Addiction and Health. https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/addiction-health (accessed 15 Feb 2026).
- American Addiction Centers. Addiction Demographics: Which Socioeconomic Groups Struggle Most? https://americanaddictioncenters.org/rehab-guide/addiction-statistics-demographics (accessed 15 Feb 2026).
- Office of the Assistant Secretary for Planning and Evaluation. Affordable Care Act Expands Mental Health and Substance Use Disorder Benefits and Federal Parity Protections for 62 Million Americans. https://aspe.hhs.gov/reports/affordable-care-act-expands-mental-health-substance-use-disorder-benefits-federal-parity-protections-0 (accessed 15 Feb 2026).
- Andrilla, C. H. A., Patterson, D. G., Garberson, L. A., Coulthard, C. & Larson, E. H. Geographic variation in the supply of selected behavioral health providers. Am. J. Prev. Med. 54, S199–S207 (2018).
- Substance Abuse and Mental Health Services Administration. Behavioral Health Barometer: United States, Volume 6. https://www.samhsa.gov/data/report/behavioral-health-barometer-united-states-volume-6
- (accessed 15 Feb 2026).
- Berwick, D. M., Nolan, T. W. & Whittington, J. The Triple Aim: Care, health, and cost. Health Aff. 27, 759–769 (2008).
- Nundy, S., Cooper, L. A. & Mate, K. S. The Quintuple Aim for health care improvement: A new imperative to advance health equity. JAMA 327, 521–522 (2022).
- Marmot, M. Social determinants of health inequalities. Lancet 365, 1099–1104 (2005).
- Compton, W. M., Thomas, Y. F., Stinson, F. S. & Grant, B. F. Prevalence, correlates, disability, and comorbidity of DSM-IV drug abuse and dependence in the United States. Arch. Gen. Psychiatry 64, 566–576 (2007).
- Compton, W. M. & Volkow, N. D. Major increases in opioid analgesic abuse in the United States: Concerns and strategies. Drug Alcohol Depend. 81, 103–107 (2006).
- Costello, E. J., Erkanli, A., Fairbank, J. A. & Angold, A. The prevalence of potentially traumatic events in childhood and adolescence. J. Trauma. Stress 15, 99–112 (2002).
- Felitti, V. J. et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. Am. J. Prev. Med. 14, 245–258 (1998).
- Livingston, J. D., Milne, T., Fang, M. L. & Amari, E. The effectiveness of interventions for reducing stigma related to substance use disorders. Addiction 107, 39–50 (2012).
- Dorsey, E. R. & Topol, E. J. Telemedicine 2020 and the next decade. Lancet 395, 859 (2020).
- Demaerschalk, B. M. et al. American Telemedicine Association: Telestroke guidelines. Telemed. E-Health 23, 376–389 (2017).
- Freeman, D. et al. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 47, 2393–2400 (2017).
- Kothgassner, O. D. et al. Virtual reality exposure therapy for posttraumatic stress disorder: A meta-analysis. Eur. J. Psychotraumatol. 10, 1654782 (2019).
- Maples-Keller, J. L., Bunnell, B. E., Kim, S.-J. & Rothbaum, B. O. The use of virtual reality technology in the treatment of anxiety and other psychiatric disorders. Harv. Rev. Psychiatry 25, 103–113 (2017).
- Wiederhold, B. K. & Riva, G. Virtual reality therapy: Emerging topics and future challenges. Cyberpsychol. Behav. Soc. Netw. 22, 3–6 (2019).
- Luxton, D. D., June, J. D. & Fairall, J. M. Social media and suicide: A public health perspective. Am. J. Public Health 102, S195–S200 (2012).
- Mariamo, A. et al. Emotional reactions and likelihood of response to questions designed for a mental health chatbot among adolescents. JMIR Hum. Factors 8, e24343 (2021).
- Concannon, D., Herbst, K. & Manley, E. Developing a data dashboard framework for population health surveillance. JMIR Form. Res. 3, e11342 (2019).
- Shanafelt, T. D. & Noseworthy, J. H. Executive leadership and physician well-being. Mayo Clin. Proc. 92, 129–146 (2017).
- Hooper, L., Doehler, K., Wallace, S. & Hannah, N. The Parentification Inventory: Development, validation, and cross-validation. Am. J. Fam. Ther. 39, 226–241 (2011).
- Cuggia, M. & Combes, S. The French Health Data Hub and the German Medical Informatics Initiatives. Yearb. Med. Inform. 28, 195–202 (2019).
- Mars, M. & Abdelsalam, M. Virtual reality and artificial intelligence in behavioral healthcare: Emerging frontiers. In Virtual Reality in Behavioral Health 145–157 (Year unknown).
- Virginia Department of Health. Drug Overdose and Substance Use. https://www.vdh.virginia.gov/drug-overdose-data/ (accessed 15 Feb 2026).
- National Institute on Drug Abuse. Overdose Death Rates. https://nida.nih.gov/research-topics/trends-statistics/overdose-death-rates (accessed 15 Feb 2026).
- City of Richmond. Opioid Response Task Force. https://www.rva.gov/human-services/opioid-response (accessed 15 Feb 2026).
- ChildSavers. Our Services. https://www.childsavers.org/services/ (accessed 15 Feb 2026).
Related Posts

Antimicrobial Resistance in Underprivileged Communities
This publication is in proud partnership with Project UNITY’s Catalyst...
Read More
Intergenerational Trauma: How a history of pain brings biological costs
Source: Nicolas Raymond, CC BY 2.0 A few years ago,...
Read More
Neuroscience, Narrative, and Never-Ending Stories
Figure 1: A field of poppies. The myths of Persephone...
Read More
Vaping and Mental Fog – The Connection Between E-Cigarette Use and Mental Function
Figure 1: Use of e-cigarette devices, like the one in...
Read More
The Growing Prevalence of Anxiety as a Public Health Issue
This publication is in proud partnership with Project UNITY’s Catalyst Academy...
Read More
Health Literacy in the United States
This publication is in proud partnership with Project UNITY’s Catalyst...
Read MoreDarius Dastur, Mishal Ali, Harshitha Ezhilarasan, Hasan Khan, Aaron Akasala